
Robert D. Stewart, MD, MPH
- Assistant Professor of Surgery
- Division of Cardiothoracic Surgery
- University of North Carolina School of Medicine
- Chapel Hill, North Carolina
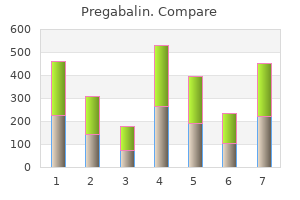
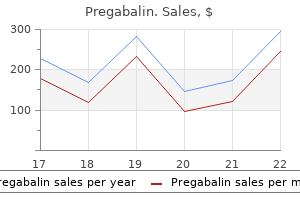
An organized internist with leadership skills can prevent or at least minimize this frustration and confusion purchase discount pregabalin online. By tracking medications prescribed by other physicians purchase pregabalin 150 mg otc, monitoring potential drug interactions 75 mg pregabalin, following up on studies or procedures per formed by subspecialists buy pregabalin uk, and responding to their recommendations purchase pregabalin 150mg with visa, the internist orchestrates multidisciplinary care and helps the patient navigate a complex sys tem of care buy pregabalin 150mg with amex. In addition, the internist acts as the patient’s advocate within the com plex health care environment of resource utilization and restricted access to care. Internists not only serve as leaders of a multidisciplinary team, but also de termine which physicians are on the playing field. As an internist you must pro vide an appropriate level of specialized care, then recognize your limitations and refer the patient to a subspecialist for optimal care. This can become a fine line for any internist—requiring an impressive breadth of knowledge but a willingness to admit limitations as well. To provide the best care, internists must learn to turn to subspecialty care when it is appropriate and establish professional, mutually respectful relationships with subspecialists. Despair, however, might be an overly dramatic descriptor for the state of general internal medicine. In recent years, studies have found that career satisfaction among general internists has de clined. Because today’s economic environment places less value on cognitive services than on procedural or diagnostic services, the decrease in the duration of individual clinic visits has compromised the man agement of psychological aspects of disease. At the same time, the growing eld erly population presents more complex comorbidities, and the traditionally val ued continuity of care has been disrupted as changes in patients’ insurance now often require a change of physician as well. There are indications, however, that advances within general internal medicine could improve job satisfaction. The option to divide inpatient and outpatient prac tice between hospitalists and primary care physicians has the potential to decrease both on-call responsibilities and total work hours. This separation of roles could also allow the outpatient-based internist more time to spend with each patient during clinic visits. Finally, the job satisfaction of all physicians depends on their ability to regain control over medical management de cisions. This would allow an internist’s time to be devoted to practicing medicine rather than constantly negotiating insurance coverage and financial reimbursement. It really de pends on whether the physician is Residency in internal medicine re a cardiologist, rheumatologist, crit quires 3 years of postgraduate ical care specialist, general in training. Cardiologists and gastroenterologists are frequently called into the hospital in accredited programs in the United the middle of the night to perform car States (excluding combined pro diac catheterizations for heart attack vic grams with other specialties). The general internist in private by both academic medical cen practice is, in a way, on call all the time. When one of their patients is admitted to the training includes experience the hospital, they receive a phone call let in both general internal medicine ting them know. It is a rig Because of the broad nature of in orous program, requiring in-house ternal medicine, residents often have a overnight call every fourth to fifth tough time responding to the question night while on an inpatient rota “Where do you intend to practice? Rotations in general patient training and even over the course of your medicine, subspecialties (consults career. Your initial career plans may be and clinic), intensive care, geri your choice during residency to pursue a atrics, and emergency medicine subspecialty fellowship or to remain in are required. For physicians demonstrate technical proficiency who choose to remain in general medi in a number of procedures, in cine, other fellowship opportunities are cluding abdominal paracentesis, available in fields such as end-of-life care, thoracentesis, central venous line medical education, and medical infor placement, and lumbar puncture. Because of the current emphasis Once a general internist is prepared on primary care, one-third of the to enter the workforce, the decision be residency must take place in an tween academic medicine and private ambulatory setting. Both have many residents spend one-half day per practice opportunities to explore. Some week in a continuity clinic where academicians are mainly educators, they manage their own panel of spending most of their time in the outpa patients over the course of 3 tient setting seeing their own patients and years. The decision to subspecial supervising residents in clinic and on the ize and apply for fellowship typi wards. Others are researchers with few in cally occurs during the second patient or outpatient responsibilities who postgraduate year. Instead, most in employment position ternists belong to a group practice such as. Some private in ternists have contracts with hospitalists to Source: American Medical Association provide all inpatient care for their pa tients, and other private internists con tinue to see patients both in the clinic and in the hospital. In both private and academic practice, the generalist initiative of the last decade gave rise to the rapid growth of a new type of internist: the hospitalist. Similar to consultants, they are called on to provide expert management for the care of sick patients admitted to the hospital wards. Typically, hospitalists do not have clinic, practice, or outpatient responsibilities. Instead of following a clinic schedule, hospitalists have a shift-work lifestyle similar to emergency medicine physicians. Patients highly benefit from having a hospitalist take care of them instead of their own private doctor coming in to round on them. With good communication be tween the two physicians, hospitalist care has been associated with lower costs, improved patient outcomes, and lower short-term mortality. In 2000, roughly half of all graduates from internal medicine residency programs sought fellowship train ing. You will still be required to have iors applying only to internal high-quality history and physical exami medicine: 1. In every subspecialty, all internists take care of very sick adult patients who have many medical problems. Allergy and Immunology Millions of people suffer from allergies, which ultimately affects their workplace productivity and results in billions of dollars lost each year. These reactions in clude respiratory diseases (asthma, sinusitis, rhinitis), adverse drug effects, and unusual skin rashes. Cardiology $287,163 A career in allergy and immunology of Endocrinolgy $166,929 fers immense intellectual satisfaction, as Gastroenterology $246,663 well as good working hours. Here, there is General Internal a strong bond between basic laboratory re Medicine $150,534 search and its clinical application. When Geriatrics $152,260 treating patients (both kids and adults), Hematology/ these specialists witness dramatic improve Oncology $210,000 ments in physical functioning. Results are Infectious Disease $166,156 usually fast, positive, and much appreci Nephrology $205,000 ated. Today, more and more people suffer Pulmonary Medicine/ from asthma and other allergic disorders. As Critical Care $213,483 such, there is an extremely high demand for Rheumatology $167,007 internists with formal training in this disci Source: American Medical Group Association pline. Career options are broad and include private practice, academics, and clinical or basic science research. Some allergist-im munologists also practice general internal medicine in addition to their subspecialty. Cardiology Like fighter pilots, cardiologists take calculated risks while exercising skill and precision. As experts in the diagnosis and management of cardiovascular diseases, they take care of life-threatening medical conditions that affect a large majority of the population. These disorders include congenital heart defects, arrhythmias, valvular problems, hypertension, and coronary artery disease. Many of the treat ment options, whether pharmacologic or interventional, have immediate life-sav ing benefits. A procedure-oriented specialty, cardiology requires a great deal of manual dexterity. You will perform cardiac catheterization, electrocardiograms, nuclear stress tests, and echocardio graphy. Due the large numbers of patients admitted to the hospital with heart attacks, cardiologists fre quently come to the hospital in the middle of the night. In the intensive care unit, they help critically ill patients maintain their blood pressure through the administration of vasopressors and other powerful drugs. Despite the rigors of the profession, cardiologists maintain long, intimate relationships with their patients. They also practice preventive medicine by identifying risk factors for early diag nosis of heart disease. If you enjoy studying the anatomy and physiology of the heart and love mastering technical procedures, then cardiology is the subspecialty for you. Endocrinology this subspecialty involves the study of hormones, endocrine glands, and their ef fects on whole-body homeostasis. You will find an intimate connection between the latest basic science research and its application in bedside clinical practice. Endocrinologists are experts in treating disease states in which glands (pituitary, thyroid, adrenal, pancreas, gonadal) are either overproducing or undersecreting hormones. These problems include diabetes, thyroid dysfunction, gonadal disor ders, pituitary tumors, adrenal gland dysfunction, and disorders of bone metab olism. Patients often live with chronic endocrine diseases that may not declare themselves for weeks or even years (other than a few subtle symptoms). Like great detectives, endocrinologists make use of an extensive array of diag nostic testing. Aside from cases of diabetic ke toacidosis, adrenal crisis, and thyroid storm, there are few endocrine emergencies. This allows the clinician ample time to think about and prepare appropriate treat ment regimens. Endocrinologists enjoy long-term relationships with their patients, who are typically on the younger side. As part of their patients’ therapy, they often have to address the behavioral and psychosocial aspects of endocrine disease. For in stance, patients with poorly controlled diabetes need to be taught (and encouraged) to modify their lifestyle, comply with their medication schedule, and use home glu cose monitoring. If you are interested in this highly scientific subspecialty with many positive outcomes, there are 2-year fellowships in endocrinology. Gastroenterology Specialists in gastroenterology treat diseases of the entire digestive system—from the esophagus to the anus, as well as the liver, gallbladder, and pancreas. De pending on the disease process, their relationships with patients may range from a single consultation. They often see patients on the surgical wards following liver transplants and in the intensive care unit with massive gastrointestinal bleeding or fulminant he patic failure. Because of the delicate nature of the subject matter, gastroenterol ogists often have to pay close attention to psychosocial aspects, particularly when discussing the implications of bowel disease for the patient’s lifestyle. As in cardiology, exciting technical procedures are an integral part of the management of gastrointestinal disorders. You will become quite adept at insert ing tubes into your patients’ mouths and rectums and seeing their diseases right before your very eyes. Colonoscopy, flexible sigmoidoscopy, and esophagogas troduodenoscopy allow the clinician to directly visualize disease, take tissue biop sies for diagnosis, and even provide immediate treatment by excising polyps or cauterizing bleeding vessels. Patients rely on their gastroenterologist to screen for precancerous lesions and to remove them before they become malignant. Whether draining fluid from an abdomen filled with ascites or recording intra esophageal pressures, there are many other diagnostic procedures. With new technology on the horizon, gastroenterologists will soon be able to perform endo luminal surgery with lasers and use built-in ultrasound probes to provide new views of our digestive organs. Gastroenterology is a perfect specialty for students who love this combination of technical interventions and cerebral challenges. Special qualifications certificates are available in hepatology (liver disease) and advanced endoscopy. Because they take a fair number of medications, geriatricians must be experts on drug interactions, ad verse effects, and how drugs are metabolized in an older person. At times, they must be selective about which diagnostic procedures and therapeutic undertak ings their patients can tolerate. Using a multidisciplinary approach, they address the physical and psychosocial needs of their patients amidst an extensive con stellation of medical issues. After all, the elderly have their own special set of prob lems, such as delirium, dementia, incontinence, and decline in functional sta tus. Geriatricians are intimately familiar with nursing home settings and dealing with Medicare. The practice options for these highly sought after specialists in clude traditional outpatient care, consultations at nursing facilities, and aca demics. Hematology–Oncology Most specialists practice both disciplines as a single field of medicine, usually with an emphasis on oncology more so than hematology. Patients with diseases of the blood, bone marrow, and lymphatic systems require the expertise of a hema tologist. These disorders include anemias, clotting abnormalities, leukemias, lym phomas, and bleeding disorders like hemophilia. Medical oncology involves the evaluation and treatment of neoplasms, both benign and malignant, of every or gan system, from the brain to the kidneys. Some oncologists develop specific ex pertise in a particular type of cancer, such as malignant mesthothelioma. They are experts on the latest forms of chemotherapy available, particularly those cur rently used in experimental clinical trials. Regardless of the area of oncology, you will no doubt acquire both a philo sophical and practical approach to life and death. Oncologists recognize that the therapy they prescribe is often harmful to the patient. They have to reconcile the benefit of every treatment option with the harm involved, which means exercis ing courage and faith in their patients’ ability to cope with the burden of disease and its treatment. This specialty, therefore, requires the highest level of sensitiv ity, compassion, and empathy.
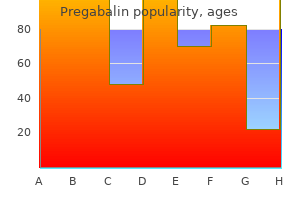
He took this discount pregabalin 75mg otc, essentially Buddhist 75mg pregabalin overnight delivery, practice and secularized it order pregabalin 75 mg with mastercard, pro viding meditation training for medical patients discount pregabalin 150 mg with amex. Kabat Zinn taught chronic pain patients mindfulness meditation discount 75mg pregabalin free shipping, and a four-year follow-up study indicated good compliance and signifcant improvement in coping with the pain (Kabat-Zinn et al order pregabalin us. He also worked with patients with anxiety disorders and witnessed signifcant reduction in anxiety at a one-year follow-up (Kabat-Zinn et al. Patients learned to identify anxious thoughts as just thoughts rather than “reality. Both studies indicate that there was an ongoing value to patients in having acquired the meditation skills. While these therapeutic practices undoubtedly have benefted thousands of peo ple, they have taught us little about the actual physiological events that occur inside the body. For instance, why is it that heart rate or blood pressure is lowered while meditating? Benson, Ornish, and Kabat-Zinn provide us with epidemiological data, that is, they give us broad pieces of information about disease and health for those who meditate as opposed to those who do not. In the previous chapter, we analyzed the major factors involved in the classic stress system. Similarly, we will now pro pose a system of hormones and neurotransmitters that make up the theta healing system—the frst system to be introduced as a coherent system of relaxation. Many endogenous ligands and the precise receptors for them are known; we can assume that there are many yet to be discovered. Neurotransmitters are both the messengers of our nervous system and the chemistry of our emotions. In some instances, the drug mimics the endogenous ligand; in other instances, it can produce a much stron ger or signifcantly different reaction than the natural chemical. Drugs can work by blocking actions of neurotransmitters or by interfering with or enhancing the mechanisms associated with the receptor, such as blocking their reuptake and preventing them from doing their job. As discussed in Chapter 1, when a drug or endogenous ligand promotes a known effect, such as relaxation at a ben zodiazepine receptor site, it is called an agonist. When a drug or endogenous ligand exhibits the ability to block a receptor, it is called an antagonist. Antagonists stop the known effects, which, in the case of benzodiazepine receptors, mean not permitting a reduction in anxiety. A third type of effect that may occur is sometimes referred to as a reverse or inverse agonist. This occurs when a drug or endogenous ligand actu ally produces an outcome that evokes symptoms opposite of those known to occur. What is quite amazing to ponder is that one receptor can interact with all three types of ligands. The communication can become more complex when multiple receptors are activated in response to an agonist. It is not only possible that different agonists for the same receptor elicit diverse magnitudes of response, but that they also select several signaling pathways (Pauwels, 2000). When it is known that a drug produces a particular effect in humans, researchers go searching to fnd a receptor into which the drug fts. As soon as the receptor is located, scientists want to know what endogenous ligand fts into the receptor. For many of the hormones, such as anandamide, which are discussed in this chapter, the receptors and endogenous ligands have been located relatively recently. Bear in mind, however, that simply fnding a molecule that binds to a known receptor does not establish that there is also a function for that ligand within the human body. As we discussed in the chapter on stress (Chapter 3), oxytocin is a hormone with properties that evoke a response that can be categorized as a relaxation response. In this chapter, we will cover properties of several other hormones that are putatively the Relaxation System 135 relaxation ligands, including benzodiazepines and associated ligands, melatonin, the cannabinoids, and N,N-dimethyltryptamine. The benzodiazepines are a class of drugs that have had enormous therapeutic impact, particularly for those individuals who have suffered from anxiety or depression. Benzodiazepines also are used for their anticonvulsant, hypnotic, and muscle-relaxing properties, and some of them are used to reduce withdrawal symptoms. They are well-known by their commercial names, such as Valium (diazepam), Xanax (alprazolam), Versed (midazolam), and Librium (chlordiazepoxide). The location of the benzodiazepine receptor was unknown for many years, yet it had to exist somewhere in our bodies because pharmaceutical companies had found drugs, which they called benzodiazepines, with distinctive anxiety-reducing thera peutic properties. Sure enough, in 1977, two teams of researchers simultaneously located specifc benzodiazepine receptors (Braestrup and Squires, 1977; Mohler and Okada, 1977). Researchers found that different types of benzodiazepines bind to the receptors with more or less potency, but the fun part was that this indeed correlated to the observed therapeutic strength of the drug—both in animals and in humans. Since that time, it has been established that benzodiazepine receptors exist in just about every tissue of the body. Eventually, it was determined that there are actually two types of benzodiazepine receptors. This action pre vents excessive discharge by reducing the potential excitability of the postsynaptic neuron (Tallman et al. So, we journey inward and observe the fow of hor monal reactions that contribute to a calming effect. In 1983, ligands for both peripheral as well as central benzodiazepine receptors were located. There are numerous ligands that have been shown to bind to the central benzodiazepine receptor. Some of the candi dates that we will review include β-carboline, nicotinamide, inosine, hypoxanthine, melatonin, and cannabinoids—all potential relaxation hormones. Curiously, in addi tion to fnding agonists and antagonists, researchers also found ligands that acted like inverse agonists, producing anxiety and convulsions, effects opposite to the ben zodiazepines (Braestrup et al. Be n zo d i a z e P i n e s a n d the im m u n e sy s The m Before surveying the putative endogenous ligands for the benzodiazepine receptor, we want to divert for a moment to share with you a little about the role of benzo diazepines in the immune system. For years, it has been known that benzodiaz epine receptors are present on platelets, monocytes, and circulating lymphocytes (Moingeon et al. Furthermore, a correlation between an imbalance of benzodiazepine receptor binding (both increased and decreased) and various diseases, including liver disease, brain tumor, epilepsy, heart disease, and leukemia, often has been cited (Basile et al. For example, research shows that diazepam modifes the immune response of rats during acute and chronic swim stress (Salman et al. This is a striking role that the benzodiazepines play in modulating the immune system—a role that we will see (later in this chapter) is also played by melatonin, the primary hormone of the pineal gland. We now proceed with a review of some of the signifcant ligands, detailing their relationship to the benzodiazepines and their role in the theta healing system. The Relaxation System 137 β-Ca r B o l i n e, hy P o x a n T h i n e, in o s i n e, a n d ni C o T i n a m i d e In 1977, when Dr. Claus Braestrup from Denmark located the benzodiazepine recep tor, he did so by locating a compound, called β-carboline-3-carboxylic acid, in the urine of mentally ill patients. It was soon learned that β-carboline inhibits brain benzodiazepine receptors, and there was much speculation that some derivative of it might be an endogenous ligand for the benzodiazepine receptor (Braestrup et al. The only problem is that the molecule that Braestrup found was not really an endogenous ligand, but an artifact of the extraction process he used to isolate it. No matter, because it turned out to be profoundly useful anyway, and soon endogenous β-carboline alkaloids were located and found to be benzodiaz epine ligands (Rommelspacher et al. These alkaloids (primarily harmane and norharmane) were also shown to possess antioxidant properties (Tse et al. However, fur ther testing uncovered its reverse agonist properties, that is, β-carboline can in fact produce anxiety and convulsions in animals and humans (Dorow et al. Because β-carboline does not share a recognition site with diazepam, researchers very early on began to specu late that the benzodiazepine receptor must be a multicomponent complex (Hirsch, 1982). In other words, it was clear that the benzodiazepine receptor site permitted numerous, diverse types of actions at its portal. Three other endogenous ligands for the benzodiazepine receptor were identi fed in the late 1970s; they are inosine, hypoxanthine, and nicotinamide (Asano and Spector, 1979; Mohler et al. Like β-carboline, they competitively bind to benzodiazepine sites, but not to other sites with similar actions, such as β-adrenergic or opiate sites. Inosine and hypoxanthine increase the inhibiting ability of diazepam, and nicotinamide was shown to potentiate the anti convulsant properties of barbiturates typically used for epilepsy (Bourgeois et al. In addition, various other factors have been proposed as endogenous ligands of the benzodiazepine receptor, such as prostaglandins and glutamate (Asano and Ogasawara, 1982; Garthwaite et al. And as mentioned, having binding properties does not mean that there is a physiological or therapeutic component. The endog enous benzodiazepine ligands appear to play a role in modulating neuronal actions, and it is my speculation that this may be the clue to their most important function (Skolnick et al. MelAtonin Melatonin (N-acetyl-5-methoxytryptamine) is the principal hormone of the pineal gland, and the pineal is our major transducer of neuroendocrine information. The pineal converts light, temperature, and 138 the Scientifc Basis of Integrative Medicine magnetic environmental information into neuroendocrine signals that infuence the body’s functioning, often via melatonin. There is an intriguing piece of research on the benzodiazepines that I happened upon over 20 years ago. The researchers discovered that melatonin not only fts into its own receptor, but also into the benzodiazepine receptor (Marangos et al. There are noteworthy similari ties between the physiological characteristics of benzodiazepines and melatonin. For example, melatonin—like the benzodiazepines—reduces anxiety, is an antidepres sant, and can aid insomnia. However, melatonin often ameliorates the same symp toms with far fewer side effects (Garfnkel et al. Diazepam can suppress melatonin-binding sites in the brain, an action that can be reversed by exogenous melatonin administration (Atsmon et al. Furthermore, when test animals are administered melatonin or a ben zodiazepine (temazepam), similar types and levels of effects. Consequently, melatonin has been used therapeutically to facilitate benzodiazepine discontinuation with insom nia patients and to enhance the reduction of anxiety in the preoperative period (Garfnkel et al. Clearly, there appears to be a reciprocal and interactive nature between these two molecules. We now know that melatonin has prophylactic functions, immune enhancing properties, and ameliorates the immune-deteriorating effects of stress. It also plays a fundamental role in immune reactions to viral and bacterial infections. The prophylactic functions of melatonin are particularly effective during times of stress. Immune system suppression in mice (including reduced antibody production, resistance to virus, gastric ulceration, and lower thymus weight) caused by the exog enous administration of the stress hormone corticosterone can actually be reversed by melatonin (Khan et al. The benzodiazepine receptors present on monocytes may be the avenue through which melatonin modu lates the immune system (Moingeon et al. Research on rodents and restraint stress reveals that the benefcial effect of melatonin is actu ally not dependent upon a reduction of corticosteroids, but rather occurs via mela tonin’s immune-enhancing capability (Maestroni and Conti, 1991). This fnding is quite stunning, as it implies that melatonin functions as an ongoing immune-system support. Reinforcing this theory are several experiments showing that the antistress effects of melatonin are only seen in mice that have been primed with antigen (Maestroni et al. Immune-enhancing func tions of melatonin also have been observed in patients with various conditions that depress the immune system, including pharmacological therapies that are typically administered for cancer treatment (Maestroni, 1993, 2001). Here again we have one of those remarkable instances of systems interacting in a bidirectional manner reminiscent of the systems integration para digms reviewed in Chapter 2 (Maestroni, 1999). So, melatonin ends up being a powerful mediator of stress that works in a subtle manner, via the immune system, perhaps synergistically with the benzodiazepines. I think that this fact alone gives us pause to suspect that it plays a part in an endog enous system of relaxation hormones. Research is just beginning to show that the stress-reducing and immune-enhancing effects of melatonin are associated with a reduction in both breast and prostate cancer (see Coker, 1999, for a review). In the chapter on the pineal gland (Chapter 10), you will read more about associations between melatonin and disease. It is as if medita tion has become part of the fabric of the lives of these individuals. In other words, there is a correlation between our physical health and the time we spend in a relaxed state of mind. Such research comes under the category of epidemiological types of studies, such as that promoted by Herb Benson and others (Benson, 1974, 1975). However, intriguingly, some newer research has shown that there is a direct correla tion between meditation and our endogenous levels of melatonin. Melatonin levels have been shown to rise during meditation and are higher in those who regularly meditate (see Figure 4. Researchers working with Jon Kabat Zinn at the Stress Reduction and Relaxation Program in Worcester, Massachusetts, found that eight women who regularly practiced mindfulness meditation (gradu ates of or teachers at the program) had higher melatonin levels (as measured by urinary 6-sulphatoxymelatonin) than did eight female controls who did not medi tate (Massion et al. Another group of researchers in Australia found that melatonin levels measured at midnight are higher immediately following a period of meditation (Tooley et al. They used experienced meditators from two dif ferent traditions, one that practiced for a half hour and the other for an hour. Both groups had signifcantly higher melatonin levels following their period of meditation than did the controls. The Australian researchers reasoned that, from a physiological standpoint, it is unlikely and undesirable that meditation during the day could cause melatonin levels to rise. Although it is speculative because the research has not been performed, I think that it is reasonable to assume that day time melatonin levels could also rise during meditation. Eyes are closed, the room is 140 the Scientifc Basis of Integrative Medicine Normal night time pattern Meditation Time figuRe 4. However, it is my contention that the slight increase in melatonin begins a hormonal cascade that we have chosen to call the theta healing system. In support of this premise is research that shows that the physiological parameters that occur during meditation are very different from those of subjects during eyes-closed rest (Jevning et al.
It was initially proposed for medical malpractice actions or products liability actions but the tactic is being employed in every type of case purchase pregabalin 75 mg line. There have been few if any cases best pregabalin 150mg, in my opinion pregabalin 75 mg for sale, where the Daubert standard would have changed the outcome discount pregabalin 150 mg amex. Utilizing Daubert will ensure that all expert opinions - including causation opinions - have some semblance of reliability buy cheap pregabalin 150 mg on-line. The Code and Rules of Evidence Committee has concluded that the Daubert statute is procedural cheap pregabalin 150mg without prescription, and will recommend, in its three-year cycle report, that the Florida Supreme Court decline to adopt Daubert as a rule of evidence to the extent it is procedural. Many motions and lengthy hearings are placing an additional and unnecessary burden on our already overtaxed court system. Daubert is too time-consuming, b d d l b li d b d f d d l id d h i i i 24a (95) 479 Please do not adopt the Daubert standard. It is an unconstitutional infringement of the separation of powers, it will result in extremely expensive hearings that take up too much court time, and it favors wealthy litigants over litigants who do not have means. Even though the Florida Supreme Court had adopted and applied the Frye standard, and had repeatedly declined to adopt Daubert as the procedure governing expert witness testimony, the legislature passed Daubert after intense lobbying efforts by special interest groups in an effort to abandon Frye in favor of Daubert. The Daubert bill, but not the amendments themselves, also includes a ‘whereas’ clause that expresses the intent to overrule the Florida Supreme Court’s decision in Marsh v. The Florida Supreme Court views Frye as a more objective test, requiring scientific evidence to be ‘generally accepted in the scientific community. Despite not being adopted by the Florida Supreme Court, and accordingly not being a rule of evidence, several courts have assumed the Daubert standard is to be applied. Multi-day ‘Daubert hearings’ essentially “trials within trials” are taking place, requiring judges to become amateur scientists, and forcing them to evaluate individual studies, look at potential error rates, and the like. Daubert puts the trial judge in the position of evaluating the science at issue, a situation which will doubtless produce different rulings, from different judges, based upon the same science. Daubert is too b d d l b l d b d f d d l d 482 There is no credible reason to change the evidentiary standard for expert witness testimony in Florida. The current standard, which has been in use in Florida State Courts for decades, has successfully achieved the desired result of screening out “junk science” no matter of which side offers it. This Frye standard ensures that scientific evidence is reliable without placing an impossible burden on judges and litigants. Not only is an attempted change unnecessary, it is detrimental to the system of justice because it makes it much more difficult, expensive and time delaying thus closing the court house doors to citizens of Florida. Bad rulings on admission of expert testimony are not corrected on appeal because of the standard of review, and trial judges thus have no incentive to keep out of their courtrooms unjustifiable expert opinions that are simply made up of whole cloth. This is a truly unfortunate state of affairs that has resulted in unwarranted and overblown jury verdicts in cases that should never have gone to a jury in the first place, and the perception-more real that imagined-that Florida courts are "judicial hellholes. The effects of this will be felt by the citizen who’s cases take longer to resolve. It will also cause there to be divergent ruling across the state, from judge to judge, which will lessen the trust the public will place in the judiciary. Jurys are more sophisticated than most give them credit, they see for themselves weak arguments and there is little risk of the so called "junk science" influencing their opinions. Daubert will only cause undue complexity in determining admissibility of expert testimony and imposes an unrealistic burden on Judges to assess scentific literature. Daubert will undoubetly lead to inconsistent rulings on the same topic undermining the integrity of our judicial system. For example, injured employees must prove that their accident was more than 50% of the cause of their injury and need for treatment. A typical example would be an employee, who has spent most of his or her working life performing arduous physical labor, suffers an low back injury in the course of their employment. This presents something of a chicken or the egg issue for the medical experts if the employee did not have degenerative arthritis, would their accident have caused the herniated disc; or conversely, but for the accident, would the employee have needed medical treatment at the present time due to the degenerative condition. There is no objective scientific formula for calculating whether the accident was more than 50% of the cause of their injury and need for treatment, and historically the medical providers and the Judges of Compensation Claims relied on the totality of the circumstances, common sense, and pure opinion to help determine whether the accident was greater than 50% of the cause. However, under Daubert, such an employee would have to present scientifically objective evidence to meet their burden of proof and, again, medical science does not provide any objective basis for determining whether the accident was more or less than 50% of the cause of the injury. If an employee cannot meet this burden, then they are not entitled to benefits under the workers compensation system, which often means that tax payers end up shouldering the expense for their on the job injury. Under the previous standard, admissibility issues seemed to be handled well, and without prolonging the process or adding to the costs of a trial. Moreover, Daubert will not assist the court in performing its gate keeping function to only allow reliable expert testimony. Rather, Daubert will significantly bog down already overcrowded state court dockets. Grid-locked state court dockets will mean that Floridians will be shut-out of the courts and unable to have courts hear their cases and controversies. This chapter/law creates an unworkable standard open to many conflicting rulings and leading to arbitrary and unintended results. Even without the formal adoption of chapter 2013-107, civil trial courts in my home circuits of Orange and Seminole counties are routinely holding multi-hour-and oftentimes multi-day hearings on expert opinions under the “new standard. Most recently my firm had an Orange County judge postpone our trial date from October 2015 to July 2016 because the judge did not have ample time available to hear the numerous Daubert challenges raised by the parties. This rule is detrimental to both plaintiffs and defendants as the court system is not equipped to handle the significant increased need for hearing times. Over the last few years, I have seen a significant increase in the number of Daubert challenges which seem to be implemented as a way to increase the cost of litigation for Plaintiffs. Once a challenge is asserted, there is no way to avoid significant time and expense, even when the subject matter of the challenge seems ridiculous. I strongly urge the Board to reject the Daubert standard if given the opportunity. Furthermore, it places an unfair burden on trial judges who will be forced to act as scientific experts in ruling on Daubert motions. There is no reason to change the evidentiary standard for expert testimony in Florida. The current standard, which has developed over many years, has been used successfully to screen out junk science which has no place in the litigation system. Ultimately, adoption of Daubert will have the effect of tilting the system in favor of litigants with extensive assets and against individual litigants. Many consumers with children are tenants in apartments who have been exposed to mold and landlords have no responsibility or accountability. This is similar to cigarette smoking approximately 50 years ago where there was link between cancer, death and smoking however the clinical evidence was not yet established. The following Florida case was one of the leading cases on the issue of mold and health until Daubert as follows: "Centex claims that the scientific principle underlying Dr. Hodgson each testified about numerous publications accepted in the scientific community recognizing the link between exposure to the highly unusual toxigenic molds and adverse health effects. Adoption of Daubert would unnecessarily burden an already overtaxed state court system. Rather, Daubert will require time consuming procedures, will produce arbitrary and varied decisions and will grid-lock state court dockets. The proposal will increase judicial time greatly and the costs of the litigation will go up. The Daubert standard ensures that only qualified experts, and reliable opinions, are presented to our juries. The Frye standard, and the "pure opinion" extension of it, was far too permissive. As a attorney who primarily practices in the realm of product liability, most of my cases are a "battle of the experts. In fact, we now live in a world of "professional experts for hire" who have honed their skills of persuasion. As such, we should do everything we can to make sure that only qualified experts, and reliable opinions, are being presented. Trial judges must have the discretion to weigh and balance the competing testimony of what the appropriate level of acceptance is in the scientific community in any given particular set of circumstances. It appears the practical reality of the situation is that the Frye standard was never truly a real problem area, in my opinion, and the legislative changes were unnecessary. Daubert will result in delay, expense, and burden on the court of having to prejudge the expert testimony. With the adoption of Daubert we can expect an avalanche of Daubert motions to be filed which will unnecessarily clog the courts, burden the judges, and delay justice. Supreme Court has stated, Frye is a more objective test, requiring scientific evidence to be ‘generally accepted in the scientific community. Daubert, however, is a multi-factorial and flexible standard, which is likely to increase confusion and conflict among the different circuits. At least one legal scholar has stated that adoption of Daubert is “more likely to produce arbitrary results than they are to produce nuanced treatment of complex questions. The Frye standard ensures that scientific evidence is reliable without placing an impossible burden on judges. Already in my personal injury practice, I have seen a challenge to expert testimony that in previous years would not have drawn any challenge. It seems that new Daubert standard has encouraged some attorneys to challenge expert testimony in circumstances where the testimony at issue is, nevertheless, well supported. While I was able to successfully get past the challenge, the cost of litigation was increased considerably by having to get expert witnesses prepared to testify at their depositions, Daubert hearings, and then trial. In my opinion, judges were doing a good job in regard to expert testimony before Daubert was adopted, and that is the way it should still be. Christopher Shakib 24a (103) 524 Daubert was a good idea but it need a lot of work. The first problem is that not every opinion, although correct, has a scientifically tested or a scientific methodology behind it, or at least not one demonstrated in the court of law. Instead of Daubert, we should allow and extra expert to scrutinize studies or methods opposing counsel is using. Moreover, I would argue that attorneys have an obligation to not mislead the court by using pseudo-scientific studies. Daubert is unfair, less objective, over burdensome, and simply not as good at the Frye test. This standard is too time-consuming, costly and difficult for under funded Florida courts to apply. Daubert increases judicial efficiency by addressing unreliable expert testimony during pre-trial stages, rather than expending substantial trial time and l h h b l l d d h h i l d d 532 533 24a (105) 534 I write to encourage the Florida Bar to recommend that the Supreme Court of Florida adopt the Daubert standard as a Rule of Evidence. I strongly believe that adopting the Daubert standard will improve the orderly administration of justice in the Florida court system by harmonizing Florida’s jurisprudence with both the federal standard and the law of most states, including those immediately surrounding Florida, and by increasing the efficiency of the judiciary. Harmonizing Florida’s Jurisprudence Since the Daubert standard’s initial adoption by the United States Supreme Court in 1993, more than 30 states have adopted Daubert in whole or in part, or incorporated its elements into the state’s facts-and circumstances assessment of reliability of expert evidence. The Court should adopt the Daubert standard to ensure clarity, reduce the uncertainty created by conflict between the legislativelyenacted law and precedent, and eliminate confusion. Moreover, Daubert will not assist the court in performing its gate keeping function, to only allow reliable expert testimony. As a result, our courts will be unable to hear the cases and controversies of Floridians. This amplifies the costs of litigation and requires a pure treating doctor to bolster his or her opinions with research into published authoritative research. No treating physician is willing to undertake such efforts merely to testify for a patient. Further, unless the injury is extremely complex, such as a traumatic brain injury without any objective radiographic findings, for example, doctors should be able to offer opinion testimony within the realm of their specialty and within the scope of their treatments. It is simple and logical and requires that, to be admissible, expert opinion must be based on facts, data, standards and conclusions that are "generally accepted in the scientific community. Daubert, on other hand, would impose an unnecessary burden on our civil justice system requiring complex multi-day hearings in almost every case merely to decide which expert opinions can be heard by a jury. A judge would have to review competing scientific studies and evaluate statistics and reams of data that would effectively permit the court to substitute its judgment for that of the relevant scientific community. More disturbingly, though, is the likelihood that perfectly reliable expert testimony would frequently be excluded. Additionally, the cost of litigation would also substantially increase both for the already overtaxed court system and also for the litigants. Parties would have to call experts often from out-of-state to testify at these mini-trials before the main trial. These monumental expenses will make resolving cases prior to trial more difficult. That "point of no return" will now be reached far earlier in the litigation process, further burdening the civil justice system with more trials that under the current regime might well have resulted in settlements. When a qualified cardiologist is prepared to testify about the generally accepted signs and symptoms of an impending heart attack, a multi-day hearing should not be required to determine whether he should be permitted to do so. While there are no shortage of lawyers, there will be shortage of lawyers who will agree to represent clients due to financial reasons. I represent a lot of Florida residents who are victims with low non-economic damages and very high economic damages. I will be forced to refuse to represent these needy individuals because it will not be financially feasible for me to accept their case. It will be cost preventative to help these victims receive justice Chapter 2013-107, Laws of Florida, (hereinafter, Daubert) amended sections 90. Even though the Florida Supreme Court had adopted and applied the Frye standard and had repeatedly declined to adopt Daubert as the procedure governing expert witness testimony, the legislature passed Daubert after several years of lobbying by special interest groups and seeks to abandon Frye in favor of Daubert. The Code and Rules of Evidence Committee has concluded that the Daubert statute is procedural and will recommend in its three-year cycle report that the Florida Supreme Court decline to adopt. Many more motions and lengthy hearings are placing an undue b d l d d i l f h b l i d 542 the Daubert standard is too time-consuming, burdensome, and costly for under resourced Florida courts to apply and amounts to an unfunded mandate. Supreme Court imposed the Daubert standard and only later did Federal Rule 702 catch up. A fortiori the Florida Supreme Court had the authority under our rule 702 to adopt Daubert as well.
In 1995 purchase pregabalin online pills, the Committee components buy pregabalin 150 mg with visa, risk from toxins and carcinogens in the diet buy pregabalin cheap online, on Clinical Practice Issues in Health and Disease of the and the impact of food processing methods that modify diet American Society for Clinical Nutrition proposed that the components discount pregabalin 75 mg without a prescription. Expertise in nutrition sci experience and formal instruction discount pregabalin 75mg online, either as a block or as an ence is achieved through graduate courses that focus on the equivalent amount of time (∼1000 hours) integrated among molecular and cellular biochemistry of foods and nutrients pregabalin 75mg with mastercard, other clinical duties over a longer time period. Approximately their relationship to human physiology, and mechanisms one-half of applicants indicated that they had completed of homeostatic regulation. The dearth of processes, (2) current medical techniques for diagnostic physicians who function as “pure” clinical nutritionists was screening, treatment, and prophylactic strategies, and (3) described over 40 years ago by van Itallie [15]andcontinues potential molecular targets for diet modifcation as adjuvant to be of concern [16]. To our knowledge, as adjuvant medical therapy, and conduct substantive trans few, if any, training programs combine knowledge of food lational clinical research. He proposed that nutrition is an integral part that candidates with doctoral training in nutrition could be of biology that deals with the physiological roles of food trained in the language and practice of medicine and in components, while the goal of dietetics is social: “to maintain clinical research methodology at the postdoctoral level. Limited training duration precluded the opportunity position to liaise with the physician and basic scientist to to conduct research and generate pilot data. Fellows were advised to write up a research proposal that wouldbeappropriateandcompatiblewiththeresourcesof 2. Patientinformation with results of imaging and diagnostic testing is presented, followed by a series of questions on the actions of dietary components in the pathophysiology. Resources include an extensive review of the literature linking nutrients with disease pathophysiology, prevention, and treatment. This resource provided development, we propose that this basic curriculum can information on diagnostic paradigms and current treatment be modifed as a model for specialized medical nutrition modalities in an organ system format. Fellows were also trained in selected use of the online institutional medical records system. Case modules were inte medicine complete with supplemental online material was grated into a guided nutritional pathophysiology tutorial that provided to each candidate for detailed discussion of medical extended throughout the 11-month fellowship. Fellows completed a series of 4 and diet history, and results of the physical examination to 6-week rotations in selected medical disciplines at the level assessment. Clinical mentors provided a lished complex cases and describe not only the presenting “hands on” introduction to patient care in their discipline and symptoms, but also comorbidities and complications. Fellows case scenario was followed by a literature review setting observed physical, laboratory, and imaging diagnostic meth forth disease processes and potential mechanisms through odsusedineachdiscipline. Links were information, participated in staf rounds and seminars, and provided to original research reports as well as meta-analyses observed selected consults and procedures during their rota andconsensusreportsthatevaluatedthestrengthofthe tion. In the course of each observership, candidates presented evidence currently available. The case modules served two actual, nutritionally informative cases to the clinical staf in purposes. They served as a nutritional pathophysiology text rounds and seminar settings and discussed diet modifca to supplement the basic pathology text and as links to tion appropriate to each patient. This respond to staf questions on both the biological plausibility information prompted the candidate to develop biological and clinical applicability of a proposed targeted modifcation. Modules served as an evaluation tool to test the interim and exit interviews with the candidate and review candidate’s understanding of the material and also revealed of the candidate’s journal, containing data on patients seen, unanswered mechanistic questions that the candidate could procedures observed, rounds attended, and the like. Candidates worked through each mentor was asked to comment on the fellowship and to module independently and presented it to program faculty assess candidate performance in the observership; see typical prior to undertaking the relevant clinical observership. At the onset of training and prior to undertaking clinical observerships, candidates (ii) Introduction to Medicine. Introduction to medical practice were required to complete online training in responsible was provided in two venues. Over the course of the clin an online tutorial on the rationale and methodology for ical observerships, candidates were expected to identify 4 Journal of Biomedical Education Table 2: Observership sites. We have also required that the online introduction to Gastroenterology medicine be completed prior to entering the Endocrinology General medicine Observership with its “hands on” introduction to medicine segments. Because we found that the medical terminology Geriatrics andabbreviationsposedachallengetosomecandidates,we Endocrinology introduced weekly interactive sessions for the candidate with Cardiology faculty mentors; these sessions have signifcantly enhanced the Fellow’s learning. R25E funds are awarded for pro Bariatric surgery gram development, not trainee support. Although trainees receive a stipend to defray part of their living expenses, this Fellows participate in rotations for four to six weeks, depending on the site. Mentors in each site have agreed to supervise Fellows at the level of awarddoesnotconstituteasalaryasdoesthetraditionalpost the third-year medical student. Tus,althoughwereceivedapplications observe procedures, participate in case discussions, and identify clinical fromanumberofhighlyqualifedandenthusiasticnewly problems with nutritional implications. Our short-term solu tion to this problem was to recruit candidates from nutrition faculty supported by their institutions during their sabbatical nutritionally related clinical problems, develop a biological year. Prospective candidates were recruited from members of plausibility for a selected study, explore appropriate clinical the Academy of Nutrition and Dietetics, specifcally from the and/or basic research methodology, and develop a protocol dietetic educators practice group. Of the four candidates trained, two familiar with research methodology used by the mentor. The candidates had undertaken heavy teaching and administra candidate was encouraged to develop collaborations with tive duties for several years afer doctorate. It is expected that the responsibilities had prevented the candidates from keeping network of mentor collaborations developed will extend past abreast of ongoing research in nutrition and medicine, the the fellowship duration and help develop the candidate’s heavy focus on nutrition pathology, medicine, and clinical research career. This barrier appears to have been surmounted by our fnal candidate who obtained her academic appointment prior to completing her 3. This permitted her to take a sabbatical Todate,wehavetrainedfourpostdoctoralfellows,allof immediately afer obtaining her doctorate. Exten some of the knowledge gaps indicated above, her research sive formative evaluation of candidate progress through the skills were more current and her progress both in the clinical curriculum revealed several barriers; we have identifed and observerships and clinical research development appeared to addressed barriers as follows. This fnal candidate was able to identify several clinical problems in (i) Prior Training. All candidates completed undergraduate need of research; she is presently developing one of these science prerequisites and graduate nutrition science training. Tese observations support the necessity toral research, several of their research topics were narrowly of full-time candidate funding for the one-year transition focusedinsomeareaofbenchnutritionscience. Some candidates (3 of 4) were credentialed as registered dietitians; (iv) Candidate Credentialing. Amajorbarrierforsomecan however, neither doctoral training nor clinical knowledge didates appeared to be a functional dichotomy between the required for dietetic credentialing includes comprehensive scope of practice of a registered dietitian and the require studyofnutritionalpathophysiologyorclinicalmedicine. Candidates indicated that their greatest years teaching dietetics, attempted to apply existing medical difculty was in following the medical considerations and nutrition guidelines to a clinical problem. It should be The authors also acknowledge the contributions of members noted that clinical mentors were very happy to access the of the New York Obesity Nutrition Research Center for dietetic knowledge and skills of the Ph. Most traditional postdoctoral Roosevelt Hospital Center for training the Fellows in the fellowships are at least two years in duration, during which language and practice of their diverse medical disciplines. While the one-year for providing insight into efective strategies for program duration of our transition training paradigm could be con development. By designating the fellowship as “transitional,” we reinforce References the concept that this frst postdoctoral year could almost be considered an extension of doctoral training. Tortoriello, “Dietary cur academic position in which he/she will conduct substantive cumin signifcantly improves obesity-associated infammation translational research. Milner, “Incorporating basic nutrition science into health medical nutrition, medical specialties, and clinical research. Finley, “Proposed criteria for assessing the efcacy of these elements in place, we propose that our intensive one cancer reduction by plant foods enriched in carotenoids, year postdoctoral fellowship curriculum can provide didactic glucosinolates, polyphenols and selenocompounds,” Annals of training and clinical experiences sufcient to transition the Botany,vol. Quon, “Mechanisms for food polyphenols to ameliorate insulin resis tance and endothelial dysfunction: therapeutic implications Conflict of Interests for diabetes and its cardiovascular complications,” American Journal of Physiology: Endocrinology and Metabolism,vol. Wong, “Diet, nutrition, and cancer prevention: the postgenomic era,” Journal of Nutrition, made major contributions to the overall research plan and vol. Merritt, “The intersociety professional nutrition education con sortium and American board of physician nutrition specialists: what have we learned? McLaren, “Nutrition in medical schools: a case of mistaken identity,” The American Journal of Clinical Nutrition,vol. Shils, “National dairy council award for excellence in medical and dental nutrition education lecture, 1994: nutrition education in medical schools—the prospect before us,” Ameri can Journal of Clinical Nutrition,vol. McLaren, “The need for physician nutrition specialists,” American Journal of Clinical Nutrition,vol. Stover, “Securing the future of nutritional sciences through integrative graduate education,” Journal of Nutrition,vol. Older adults are more susceptible to foodborne infections than younger adults and many older adults do not follow recommended food safety practices. Following program exposure, many of the respondents advised their older adult patients about food safety. The fndings from this study suggest that the program is a useful tool that can assist those who provide nursing care as they interact with their older patients and lead them to positively infuence older adults’ food safety practices. However, more research is needed to examine changes in providers’ behaviors as a result of program exposure and the accompanying efect on older adults’ food safety practices. Tese practices include avoiding foods that are more To build healthy eating patterns, the 2010 Dietary Guidelines likely to be contaminated with pathogens such as raw or for Americans recommends that all people follow food safety undercooked eggs; raw or undercooked meat, poultry, or recommendations when preparing and eating foods to reduce seafood; hot dogs and deli meats that have not been reheated the risk of foodborne illnesses [1]. Older adults are at a greater to steaming hot; sof cheeses made from unpasteurized milk; risk for developing serious complications from foodborne raw sprouts; and unpasteurized milk and juices; using an infections compared with younger adults [2–5]. Factors such appliance thermometer to ensure the refrigerator’s ambient ∘ as decreased stomach acid production, intestinal motility, temperature is 40 F or less; using a food thermometer to malnutrition, immobility, chronic diseases, living in a nursing check the internal temperature of meat and poultry dishes; home environment, and increased use of antibiotics cause refrigerating food promptly; and other practices. However, older adults to be more susceptible to foodborne infections research suggests that many older adults may not be following [5, 6]. Listeria monocytogenes that most likely originated from con A nationally representative survey of older adults [11]and taminated cantaloupes. According to the Centers for Disease a study conducted by Boone and colleagues [12]revealedthat Control and Prevention, among the 72 ill persons afected by seniors would prefer to learn about food safety from their theoutbreakmostwereaged60orolderorhadweakened health care providers. A few resources have been developed to communicate 2 Journal of Biomedical Education Table 1: Booklet sections. Section Topics covered Reasons older adults are susceptible to foodborne infections, symptoms (1) Learn about Foodborne Illness associated with foodborne illness, and caring for someone with foodborne illness (2) Foods Seniors Outgrow Foods older adults should avoid eating to prevent foodborne illness (3) Food Storage 101 Recommended storage times for foods and how to safely store lefovers Tools needed to maintain a sanitary kitchen and tips such as using an (4)TeRightToolsforaSpotlessKitchen appliance thermometer to ensure the refrigerator’s temperature is 40 Fo∘ r below Safe hand washing, sanitation, and food hygiene practices. Additionally, we disseminated booklets and recruited edge, none have specifcally been tailored to nurse-older adult individuals for the study at local conferences, including the patient communications about food safety. Tennessee Nurse’s Association and Tennessee Association of The aim of this study was to implement the Food Safety Student Nurses Joint Convention and the Tennessee Public Because You Care! Intervention, a program developed for Health Association’s Annual Education Conference. Study those who provide nursing care for older adult patients and to participants were required to care for patients aged 60 or assess participants’ response to the program. The intervention older and be a nurse practitioner, registered nurse, licensed was an educational booklet developed by Tennessee State practical nurse, or certifed nursing assistant. University that provided information tailored to nurse-older adult patient communications about foodborne illnesses and 2. This study examined participants’ afer the booklets were disseminated, we administered the opinions of the booklet and whether the booklet motivated survey via the participant’s preferred method: Web or tra them to share the booklet with others or provide food safety ditional pen-and-paper method. Inter provided digital copies of the booklets via e-mail were told vention is a 47-page educational booklet that includes food they would be contacted again about a week afer receiving safety tips and quizzes intended for older adults and those the booklet and provided with the survey Web link. The The survey collected information on participants’ opin booklet uses a large font size, large colorful graphics, and ions of the booklet, current food safety knowledge, and any nontechnical language so that older adults with failing changes made following exposure to the intervention. The booklet is currently accessible tutional Review Board, and all study participants were fnan online at fnic. A total of 88 individuals retrospective survey without a control or comparison group. For 77% Using convenience sampling, we recruited study participants of the respondents, more than 50% of their patients were aged from June to December 2011 using the following methods: (1) 60 or older. Fify-fve percent of the respondents were regis placing advertisements in the American Nurses Association tered nurses, and 43% of the respondents specialized in geri e-newsletters, (2) posting study recruitment announcements atrics. The majority of the respondents worked in long-term Journal of Biomedical Education 3 Table 2: Respondents’ opinions of the booklet (= 88). Table 2 describes respondents’ dents, 40% reported that they frequently or very frequently impressions of the booklet. Seventy-three percent of the provide food safety information to their older adult patients. Seventy-four percent reported that they did recommended practices for handling and preparing food allormostofthequizzesinthebooklet. Afer Over 90% of respondents agreed that afer reading the book reading the booklet, 57% of respondents reported that they let they were better prepared to advise older adults and/or advised their patients not to eat certain foods because of con their caregivers to safely prepare food and that they were more cerns about food safety, and 57% of respondents reported that aware of food safety. More than half of respondents agreed they gave their patients recommendations on how to safely that the booklet showed them that they did not know enough store, handle, or prepare food at home. Respondents who about properly preparing food for older adults, and 24% of reported providing these recommendations to their patients respondents agreed that the booklet was too lengthy. Responses to the cent of respondents reported that they fled the booklet or put opened-ended questions are provided in Table 3. Nearly two-thirds of their patients (nine respondents skipped the 4 Journal of Biomedical Education Table 3: Respondents’ recommendations to their patients as a result of reading the booklet. What foods have you advised your patients aged 60 or older not to eat based on what you learned in the booklet? Discussion/Conclusions poultry (24%); and mold-ripened, blue veined, or sof cheeses (20%). Among respondents who described recommenda The nurses and other care providers surveyed had favorable tions they had given their patients for safe food storage, han impressions of the booklet and believed that it better prepared dling, or preparation (=41) (nine respondents skipped the them to advise older adults and/or their caregivers on rec question or did not provide a legible response), almost a third ommended food safety practices. Based on the results of the recommended proper storage times for refrigerator foods survey, the booklet appeared to motivate respondents to or recommended other storage practices not already spec educate older adult patients about food safety. Education con ifed, including storing pantry items in closed containers, sisted of advising older adult patients not to eat certain “risky” setting the freezer at the proper temperature, or storing frozen foods or advising patients on how to safely store, handle, or foods for the proper amount of time. The booklet also led The booklet recommends that older adults use an appli some respondents to recommend that patients use appliance ance thermometer to monitor their refrigerator’s temperature thermometers to ensure that perishable foods are stored at ∘ and a food thermometer to check meat and poultry dishes 40 F or below or recommend that patients use food ther for doneness.
The external reality of demons was almost entirely unques tioned from antiquity through late medieval times pregabalin 75 mg low price. Maimonides denied their reality pregabalin 75mg free shipping, but the overwhelming majority of rabbis believed in dybbuks purchase pregabalin 150mg on-line. Of Credulity and Incredulity discount pregabalin 150mg free shipping, that witches must exist because purchase pregabalin with mastercard, after all order pregabalin paypal, everyone believes in them. The Pope appointed Kramer and Sprenger to write a compre hensive analysis, using the full academic armoury of the late fifteenth century. Little attention is given to the possibility that accusations might be made for impious purposes jealousy, say, or revenge, or the greed of the inquisitors who routinely confiscated for their own private benefit the property of the accused. In any case, it was nearly impossible to provide compelling alibis for accused witches: the rules of evidence had a special character. As a result pubic hair was shaved, and the genitalia were carefully inspected by the exclusively male inquisitors. No one knows how many were killed altogether perhaps hundreds of thousands, perhaps millions. Those responsible for prosecuting, torturing, judging, burning and justifying were self less. In such a case, explained the witch judge Pierre de Lancre (in his 1612 book, Description of the Inconstancy of Evil Angels), the Catholic Church would be committing a great crime by burning witches. Heresy was a still more serious crime, and both Catholics and Protestants punished it ruthlessly. But if people could actually read the Bible in their own language instead of arcane Latin, they could form their own, independent religious views. Such a cast of mind, such a climate of absolute confidence that knowledge should be rewarded by torture and death were unlikely to help those accused of witchcraft. Burning witches is a feature of Western civilization that has, with occasional political exceptions, declined since the six teenth century. Unless we believe that demons really exist, how can we understand so strange a belief-system, embraced by the whole Western world (including those consid ered the wisest among us), reinforced by personal experience in every generation, and taught by Church and State? The culture myths of ancient Greece and Rome told of gods appearing to women as bulls or swans or showers of gold and impregnating them. In one early Christian tradition, philosophy derived not from human ingenuity but out of demonic pillow talk, the fallen angels betraying the secrets of Heaven to their human consorts. In an epoch of demon hysteria, it was easy enough to demonize those we feared or hated. Occasionally an entire people for example the Huns or the inhabitants of Cyprus were accused by their enemies of having been sired by demons. In 1645 a Cornish teenager, Anne Jefferies, was found groggy, crumpled on the floor. Sometimes the young man was convinced the entire business was a dream; other times he was certain he was awake. In modern times [Gibbon is writing in the middle eight eenth century], a latent and even involuntary scepticism adheres to the most pious dispositions. They felt, or they fancied, that on every side they were incessantly assaulted by daemons, comforted by visions, instructed by prophecy, and surprisingly delivered from dan ger, sickness, and from death itself, by the supplications of the church. The imagination, and even the senses, were deceived by the illusions of distempered fanaticism; and the hermit, whose midnight prayer was oppressed by involun tary slumber, might easily confound the phantoms of horror or delight which had occupied his sleeping and his waking dreams. But by 1628, James had become a thoroughgoing sceptic mainly because adolescents had been found faking demonic possession, in which state they had accused innocent people of witchcraft. I still remember that thing crouching there, so terribly ugly, its arms and legs like the limbs of a great insect, its eyes glaring at me. Typically, Lindsey ignores verse 32 in which Jesus makes it very clear he is talking about events in the first, not the twentieth, century. The Bible nowhere explicitly affirms or negates intelligent extraterres trial life. Implicitly, however, Scripture does deny the exist ence of such beings, thus also negating the possibility of flying saucers. He concludes: Science may have evicted ghosts and witches from our beliefs, but it just as quickly filled the vacancy with aliens having the same functions. Soon it takes on a life of its own, inspires others trying to understand their own visions and halluci nations, and enters the realm of folklore, myth and legend. The connection between the content of spontaneous temporal lobe hallucinations and the alien abduction paradigm is consistent with such a hypothesis. They are ordered to assassi nate a political leader or a folk hero, or defeat the British invaders, or harm themselves, because it is the wish of God, or Jesus, or the Devil, or demons, or angels, or lately aliens. Think of the power of repetitive imagery in advertising, especially to suggestible viewers and readers. Somehow small hairless beings with big heads (and eyes) have been our staple aliens for a long time. Wells argued that humans evolved from smaller-brained but hairier primates with an athleti cism far exceeding that of Victorian academics; extrapolating this trend into the far future, he suggested that our descendants should be nearly hairless, with immense heads, although barely able to walk around on their own. It looks to me eerily like a foetus in roughly the twelfth week of pregnancy, or a starving child. Not a single being presented in all these accounts is as astonishing as a cockatoo would be if you had never before beheld a bird. Samuel Butler, Characters (1667-9) or just an instant in the darkened room I sense an apparition Fcould it be a ghost? In astonishment, I seem to be smelling the salt air of the Coney Island summer seashore of my childhood. In an obsessively rigid, practically ori ented society, perhaps I would be cautious about admitting to such experiences. Courts have banned its use as evidence or even as a tool of criminal investiga tion. The American Medical Association calls memories surfacing 130 On the Distinction between True and False Visions under hypnosis less reliable than those recalled without it. True, Lawson had cued his subjects briefly and directly; but in many cases the therapists who routinely deal with alien abductions cue their subjects, some in great detail, others more subtly and indirectly. The psychiatrist George Ganaway (as related by Lawrence Wright) once proposed to a highly suggestible patient under hypnosis that five hours were missing from her memory of a certain day. There are many other examples, some a spurious memory of being lost as a child in a shopping mall, for instance of greater emotional impact. False memories can be implanted even in minds that do not consider themselves vulnerable and uncritical. The child who, when first asked, cor rectly denies having caught his hand in a mousetrap later remem bers the event in vivid, self-generated detail. Is there any reason to think that adults are wholly immune to the fallibilities exhibited by children? On many occasions in his Presidential campaigns, Mr Reagan told an epic story of World War Two courage and sacrifice, an inspiration for all of us. Only it never happened; it was the plot of the movie A Wing and a Prayer that made quite an impression on me, too, when I saw it at age 9. It is not hard to imagine serious public dangers emerging out of instances in which political, military, scientific On the Distinction between True and False Visions or religious leaders are unable to distinguish fact from vivid fiction. Or it may no longer correspond, even in its major features, to what really happened. If we sew cleverly enough, we have made ourselves a memorable story easy to recall. The situation is rather like the method of science itself where many isolated data points can be remem bered, summarized and explained in the framework of a theory. In science the theories are always being reassessed and con fronted with new facts; if the facts are seriously discordant beyond the error bars the theory may have to be revised. But in everyday life it is very rare that we are confronted with new facts about events of long ago. More than gods and demons, the best-attested apparitions are those of saints, especially the Virgin Mary in Western Europe from late medieval to modern times. Christian Jr in his book Apparitions in Late Medieval and Renaissance Spain (1981). Alternatively, in plague-infested times, Mary promises to cure the disease but only if her request is satisfied. But when she informs her father or husband or priest, she is ordered to repeat the story to no one; it is mere female foolishness or frivolity or demonic halluci nation. Days later she is confronted again by Mary, a little put out that her request has not been honoured. In one case the testimony of a delirious eight-year old boy, taken two days before his death from plague, was soberly accepted. Thus anyone seeing a vision disturbing to those in power was ipso facto an unreliable witness, and saints and virgins could be made to say whatever the authorities wanted to hear. The fervour of pilgrims in such shrines was impressive; it was not uncommon for rock scrapings or dirt from the shrine to be mixed with water and drunk as medicine. Almost all the urgent requests by Mary were remarkable for their prosaicness for example, in this 1483 apparition from Catalonia: I charge you by your soul to charge the souls of the men of the parishes of El Torn, Milleras, El Salent, and Sant Miquel de Campmaior to charge the souls of the priests to ask the people to pay up the tithes and all the duties of the church and restore other things that they hold covertly or openly which are not theirs to their rightful owners within thirty days, for it will be necessary, and observe well the holy Sunday. The matter was addressed in the Siete Partidas, the codex of canon and civil law compiled under the direction of Alfonso the Wise, king of Castile, around 1248. In it we can read the following: Some men fraudulently discover or build altars in fields or in towns, saying that there are relics of certain saints in those places and pretending that they perform miracles, and, for this reason, people from many places are induced to go there as on a pilgrimage, in order to take something away from them; and there are others who influenced by dreams or empty phantoms which appear to them, erect altars and pretend to discover them in the above named localities. In listing the reasons for erroneous beliefs, Alfonso lays out a continuum from sect, opinion, fantasy and dream to hallucination. Clearly, the secular and ecclesiastical authorities, even in times of extreme credulity, were alert to the possibilities of hoax and delusion. From which could follow the seduction of peoples, the inception of new sects, and many other impieties that subvert the Church and Catholics. For poor peasants whose visions had no political content, the punishments fell short of the ultimate severity. But in deference to certain just reasons that move us to mitigate the rigour of the sentences we decree as a punish ment to Francisca la Brava and an example to others not to attempt similar things that we condemn her to be put on an ass and given one hundred lashes in public through the accustomed streets of Belmonte naked from the waist up, and the same number in the town of El Quintanar in the same manner. And that from now on she not say or affirm in public or secretly by word or insinuation the things she said in her confessions or else she will be prosecuted as an impenitent and one who does not believe in or agree with what is in our holy Catholic faith. Despite the penalties, it is striking how often the witness stuck to her guns and, ignoring the encouragements offered her to confess 138 On the Distinction between True and False Visions that she was lying or dreaming or confused, insisted that she really and truly had seen the vision. In a time when nearly everyone was illiterate, before news papers, radio and television, how could the religious and icono graphic detail of these apparitions have been so similar? William Christian believes there is a ready answer in cathedral dramaturgy (especially Christmas plays), in itinerant preachers and pilgrims, and in church sermons. People sometimes came from a hundred miles or more so that, say, their sick child could be cured by a pebble that had been trodden on by the Mother of God. In a time haunted by drought, plague and war, with no social or medical services available to the average person, with public literacy and the scientific method unheard of, sceptical thinking was rare. The content of the communication is, despite its purported celestial origin, mundane. The witnesses, often females, are troubled about speaking out, especially after encountering ridicule from males in positions of authority. In I Am With You Always: True Stories of Encounters with Jesus (Bantam, 1995), first-hand accounts, some moving, some banal, of such encounters are laid out. If you dreamed it, if it felt good, if it elicited wonder, why then it really happened. Note there are no therapists touting the reality of needles in cans and urging their patients, subtly or directly, to go public with the news. Insensibly one begins to twist facts to suit theories, instead of theories to suit facts. Why do they believe these witnesses but not those who reported, with comparable conviction, encounters with gods, demons, saints, angels and fairies? Moreover, such experiences were likely to be generated and interpreted as real events rather than imagin ings when they were associated with restricted sensory envi ronments. What a more critical mind might recognize as a hallucination or a dream, a more credulous mind interprets as a glimpse of an elusive but profound external reality. Therapists who take the alien abduction stories at face value deny this, saying they would know if their patients were sexually abused. Some estimates from opinion surveys range as high as one in four American women and one in six American men have been sexually abused in childhood (although these estimates are prob ably too high). It would be astonishing if a significant number of patients who present themselves to alien abduction therapists had not been so abused, perhaps even a larger proportion than in the general population. Both sexual abuse therapists and alien abduction therapists spend months, sometimes years, encouraging their subjects to remember being abused. I find it striking that alien abduction therapists find so few cases of sexual abuse and vice versa. Those who have in fact been subjected to childhood sexual abuse or incest are, for very understandable reasons, sensitive about anything that seems to minimize or deny their experience. Compelling physical evidence photos, for example, or diaries, or gonorrhoea or chlamydia in the child have in some cases come to light. Rape victims are ten times more likely than other women to use alcohol and other drugs to excess. While there is better reporting today than in the past, there does seem to be a significant increase in cases of child abuse reported each year by hospitals and law enforcement authorities, rising in the United States ten-fold (to 1. Perhaps increasing publicity given to contemporary cases of child abuse emboldens adults to remember and focus on the abuse they once suffered. The Emory University psychologist Ulric Neisser says: There is child abuse, and there are such things as repressed memories. But there are also such things as false memories 146 Therapy and confabulations, and they are not rare at all. They are still more likely to occur in cases where suggestion is a lively possibility, where memories can be shaped and re-shaped to meet the strong interpersonal demands of a therapy session. And once a memory has been reconfigured in this way, it is very, very hard to change.