
Sarah Gamble PhD
- Lecturer, Interdisciplinary

https://publichealth.berkeley.edu/people/sarah-gamble/
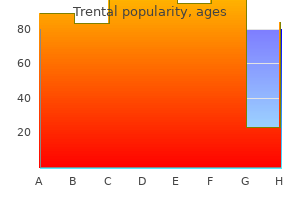
Exhibit 113 Drug Com binations and Com m on Reasons for Use Combination Reasons Heroin plus alcohol Enhance a high; create euphoria or sedation Heroin followed by alcohol Medicate opioid withdrawal; medicate cocaine overstimulation rheumatoid arthritis exhaustion purchase 400 mg trental free shipping. Other interventions have are a major cause of death among patients in met with limited success arthritis in hip purchase discount trental on-line. Eighty percent of these patients com tal disorders arthritis in feet and legs cheap trental 400mg with visa, greater criminality psoriatic arthritis diet coffee 400 mg trental free shipping, and poorer plied with treatment requirements and com social and family functioning and peer relations pleted treatment (Kipnis et al rheumatoid arthritis quality of life questionnaire pdf purchase generic trental online. High alcohol problems in the previous 6 months dose benzodiazepines can cause serious prob (Appel et al arthritis in knee yahoo trental 400 mg visa. These risks ation between inadequate methadone doses and are potentiated when high doses of benzodi increased cravings for both heroin and alcohol. Regular benzodiazepine use respiratory effects (perforation of nasal septum, for 3 months or more may be associated with bronchial irritation) if inhaled or smoked, or physiologic dependence, even when benzodi mental effects (anxiety, depression, anger, azepines are taken in prescribed doses. The combi glutethimide are more likely than benzodi nation of alcohol and cocaine is popular azepines to produce lethal overdose because because it can create a more intense high and people who abuse them develop tolerance for less intense feelings of inebriation than either their sedative and euphoric effects but not for substance alone. Therefore, temper discomfort when they come down from as these people increase their dosages to get a cocaineinduced high. People who are opioid addicted more difficult to engage and retain in treatment and abuse nonbenzodiazepine sedatives usually than patients who do not abuse all three sub need inpatient detoxification before starting stances (RowanSzal et al. The combination of alcohol and phine metabolism (see chapter 3), and can cocaine tends to have exponential effects on make stabilization difficult. The mix withhold treatment medication for patients who ture of opioids, cocaine, and alcohol can be appear intoxicated with a sedativetype drug lethal and has been identified as a leading cause until intoxication has cleared and patients are of accidental overdose (Coffin et al. Nonbenzo cocaine use appeared to lower the methadone diazepine sedative and barbiturate abuse is concentration in blood. These medications are less patients reduced their cocaine use when their widely abused than in the past, because benzo methadone dosages were increased. Borg and diazepines are less dangerous and easier to colleagues (1999) found that adequate doses of obtain in many areas. Nicotine 2000) and that disulfiram also was promising Tobacconsmokingrelated illnesses are a major for patients treated with buprenorphine cause of morbidity and mortality among (George et al. Patients tion, because effective medications are available, who continue using illicit drugs sometimes tobacco cessation should be a regular part of erode the morale of other patients, who may patientsi treatment plans. Abuse of other substances declaring the nonopioid abuse in along with opioid addiction presents many studies reported by problems and challenges for treatment desirability of Borg and colleagues providers and patients. W ithout treatment, a (1999) and by person with these problems may continue crim cessation of all Tennant and inal activity; remain obsessed with substance Shannon (1995). In addition, some State regulations set chapter 8) and only when staff members have specific timetables for compliance, although the exhausted all reasonable alternatives. Usually patients who abuse multiple substances require a more intensive Dosage Adjustm ents level of care for a limited period. Patients may be to a therapeutic community, residential treat abusing other drugs to selfmedicate withdraw ment, or other longterm, more structured and al symptoms caused by inadequate dosages or controlled environment. Use of cocaine and other sub counseling is associated with a reduction in stances should cause concern because it under opioid and other substance use by patients in mines patient stability. In a study of patients who abused multi as less serious unless clear evidence exists of ple substances and had cooccurring disorders impaired functioning. Changing such attitudes and behav reduced their cocaine use more than those in iors requires patience and effort. These policies who received additional cognitive behavioral should clarify any ambiguity about abstinence therapy for cocaine abuse and patients who from nonprescribed medications but encourage received standard methadone treatment, therapeutic use of medications that are Treatm ent of M ultiple Substance Use 187 cocaine use declined significantly for both loss of consciousness, lifethreatening with groups (Magura et al. This type of withdrawal is not treatable with methadone Increased Drug Testing (Sporer 1999; W hite and Irvine 1999). In addition, a history of seizures or toxic psychosis during Inpatient withdrawal from a sedativehypnotic or anxi olytic drug or from alcohol is an absolute Detoxification and indication for inpatient detoxification. However, mental health and addiction treatment systems often are In this separated. This situation may result in patientsi being treated at one location for addiction and at another for mental disorders. These problems, along with uncertainties about effec CoOccurring tive interventions for patients with both addiction and mental disorders, Disorders have stimulated research in this area. Etiology of the consensus panel acknowledges that other types of disorders also CoOccurring occur with substance use disorders, such as cognitive and medical disor Disorders ders and physical disabilities. These symptoms may indicate either underlying cooccurring disorders that would be present regardless of substance Factors Affecting Prevalence use. Numerous studies have indicated However, some of these studies did not that rapid, accurate identification of patientsi determine whether symptoms of cooccurring cooccurring disorders and immediate interven disorders were related to the pharmacological tions with appropriate combinations of psychi effects of substances or to an underlying atric and substance addiction therapies improve nonnsubstancerelated disorder. Community surveys from both indicated that female patients receiving the Epidemiologic Catchment Area study and methadone were more likely than male patients the National Comorbidity Study found that, to have psychotic and affective disorders among respondents with substance use disor (Calsyn et al. M otivation for Etiology of Treatm ent and CoOccurring Disorders CoOccurring Disorders Mueser and colleagues (1998) identified four common models to explain the relationship Some studies have found that cooccurring dis between cooccurring and substance use orders motivated people who were addicted to disorders: Treatm ent of CoOccurring Disorders 191 i Primary substance use disorder and factors, such as poverty, social isolation, drug secondary cooccurring disorder. This availability, or lack of accountability by adult idisease modeli holds that substance use dis caregivers, also contribute to both substance orders cause most cooccurring disorders in use and cooccurring disorders through a patients. Appropriate treatment, by this the complex interaction between environment ory, focuses on the underlying substance use. The bidirectional i Primary cooccurring disorder and sec model has not been evaluated systematically. This iselfmedicationi model, proposed by Screening for Khantzian (1985), argues that preexisting mental disorders are a significant cause of CoOccurring Disorders substance use disorders. People who are drug the consensus panel believes that admission addicted choose drugs that lessen painful and ongoing assessment routinely should incor feelings caused by their mental disorders, porate screening for cooccurring disorders. A adequate treatment of the psychopathology negative result generally should rule out imme resolves the substance use disorder. This model holds that detailed assessment by a trained professional shared genetic or environmental factors may (see chapter 4). Questions questions during initial intake and defer about trauma should be brief and general, other questions until applicants are no longer without evoking details that might precipitate intoxicated or in withdrawalobut wait no stress. If indications of a cognitive impairment are i W hich staff members to consult if questions present, a mental status examination should arise about these procedures or the results. Screening for cooccurring disorders usually entails determining Screening for cognitive i An applicantis immediate safety and self im pairm ent control, including any suicide risk, aggres the accuracy of instruments to screen for sion or violence toward others, or domestic cooccurring disorders may be compromised if or other abuse or victimization and the administered to patients with cognitive impair ability to care for himself or herself (see ments. Questions understanding information in their first lan about the relationship of mental disorders guage. Disorders: Clinical Descriptions and Diagnostic Guidelines (W orld Health Organization 1992). Other important considerations in selecting a screening tool for cooccurring dis Although many insurance companies require orders include its psychometric properties and International Classification of Diseases diag cultural appropriateness and, if the test is self nostic codes for reimbursement purposes, administered, the literacy level required. M aking and Confirm ing Substanceinduced a Psychiatric Diagnosis cooccurring disorders After a possible cooccurring disorder is identi Substanceinduced cooccurring disorders are fied during screening, an experienced, licensed associated with intoxication, withdrawal, and mental health clinician. Substance use can magnify 122 shows the association between substance symptoms of independent cooccurring induced cooccurring disorders and substances disorders. It is noteworthy that different drugs heighten the mood have been associated with different types swings of bipolar dis of cooccurring disorders and that some order; intensify the [I]ndependent and (such as opioids) have relatively few or no hallucinations and reported psychotoxic effects, whereas others paranoid delusions have many. A definitive diagnosis often Careful assessment including a family history must wait until a patient is stabilized on treat is critical to determine whether presenting ment medication for a minimum of 5 to 7 days symptoms indicate independent cooccurring (but preferably 2 to 4 weeks) and any continu disorders or disorders induced by substance ing substance use is eliminated. Although use or a general medical or neurological several weeks of abstinence may improve the condition. In many cases, people who abuse accuracy of diagnoses, symptoms of severe multiple substances have both an independent cooccurring disorders. In addition, I indicates that the specifier W ith Onset During Intoxication may be noted for the category; W indicates that the specifier W ith Onset During W ithdrawal may be noted for the category (except for W ithdrawal Delirium); and I/W indicates that either W ith Onset During Intoxication or W ith Onset During W ithdrawal may be noted for the category. Research has suggested that persons tain whether a cooccurring disorder is primary with cooccurring disorders are at higher risk or secondary: of suicide, psychiatric hospitalization, legal difficulties and incarceration, homelessness, i Label the disorder according to predominant lifethreatening infectious diseases, domestic symptom pattern and specified criteria. Patients with more than one Conversely, a review by Drake and Brunette cooccurring disorder engaged in treatment (1998) concluded that substance abuse compli more readily than those who were addicted cates cooccurring disorders, often precipitat only, and both groups were similar in average ing relapse to psychopathological symptoms, incidence of drug use or criminal activity. Despite these limita believes that cooccurring disorders can tions, numerous studies have found that many improve substantially but that outcomes patients with cooccurring disorders did well depend heavily on additional treatment being when appropriate psychiatric and substance provided for these disorders and that patients abuse treatments were delivered. The consen with severe symptoms may require longer, sus panel recommends more intensive and more intensive treatment. Early studies found that the severity cent of people seeking treatment for opioid of cooccurring disorder symptoms, particular addiction (Brooner et al. The consensus panel special attention paid to depression and suici believes that the best strategy is to stabilize dal ideation (Villagomez et al. Treatm ent of CoOccurring Disorders 199 the condition that is most severe and threaten oxazepam (Seraxfi) rather than lorazepam, ing, it usually is best to address all of a patientis clonazepam, alprazolam or diazepam. Educating patients about co disorders should Treatment for occurring disorders helps. Remission of cooccurring planning and imple tion from admis disorder symptoms should be an important mentation for this secondary goal. Physicians should be careful about drugs, benzodiazepines, or other sedatives may prescribing substances with abuse potential, be required to establish behavioral control such as benzodiazepines. Exceptions include patients who have with the lowest abuse potential for their condi acute, substanceinduced disorders such as tion. People with psychiatric treatment histories, or verified cooccurring disorders, particularly depression diagnoses and current prescriptions for medi or dysthymia, were more likely than those with cations to treat such disorders (regardless of out Axis I disorders to continue needle sharing whether they are used) should continue or and other highrisk behaviors (Camacho et al. Treatm ent of CoOccurring Disorders 201 M odels of Care Risk factors and predictors for Although it is not always feasible to provide suicidal ideation and threats more specialized services on site, patient adher People who are opioid addicted have high rates ence to medical treatment was found to drop of suicide and attempted suicide, ranging from dramatically when such services were provided 8 to 17 percent in some studies with even higher through offsite referral (Batki et al. Substance intoxication or withdrawal noncompliance may have significant conse can cause or exacerbate suicidal ideation or quences for personal, social, and public health. Chapter 4 dis If a program cannot provide onsite ancillary cusses risk factors for suicide and recommend services, it is important that staff members ed treatment responses. Risk factors do not identify cooccurring disorders early so that predict individual behavior, but a highrisk they can refer patients to appropriate profile merits immediate and ongoing attention resources. In an early work, attempts or difficulty controlling violent behav Kosten and Rounsaville (1988) found that acci ior during their lifetimes (Cacciola et al. More recently, Darke and selves or others or have psychotic symptoms or Ross (2001) reported that 92 percent of disordered thinking that could interfere with patients who overdosed characterized the their safety or that of others should receive overdose as accidental. In that study, of the 40 immediate, aggressive intervention on admis percent who acknowledged a previous suicide sion and throughout treatment. Staff members attempt, only 10 percent deliberately overdosed should be trained to notice indications of with heroin compared, for example, with 21 suicidal or homicidal risks. These observations percent who deliberately overdosed with should be documented and communicated to benzodiazepines. This is 202 Chapter 12 important for patients who appear withdrawn, other mood stabilizers or antidepressants take depressed, angry, or agitated or are known to hold, which can take several weeks. Medication have experienced a recent significant loss or assisted treatment of acute suicidality should be other source of stressoespecially if a co on an inpatient basis unless family members or occurring disorder is suspected or diagnosed or friends are willing to be responsible for adminis if a patient still is intoxicated or withdrawing tering the drugs regularly, keeping the atrisk from a psychoactive substance. Some key factors in this decision are clearly To aid in screening and referral for suicidality expressed intent, specific and lethal plans, and homicidality, all programs should have accessible means, limited social or familial protocols in place that specify resources, severe symptoms of mental illness or psychosis, command hallucinations, hopeless i W ho asks what questions or uses what ness, and previous suicide or homicide attempts. Programs should encourage participation in Decisions should be made about using antipsy mutualhelp groups that focus on the needs of chotic medications, benzodiazepines, or other people with cooccurring disorders. Exhibit 12 sedatives to establish behavioral control rapid 3 lists some of the best known of these groups, ly (Minkoff 2000). Patients can patients attend daily (at least in the early stages explore relevant themes by emphasizing positive of treatment) and onsite physicians and other coping strategies and sharing experiences. Exhibit 124 Topics for Psychoeducational Groups for People W ith CoOccurring Disorders i Causes, symptoms, and treatment for substance use and cooccurring disorders i Medical and mental effects of cooccurring disorders i Psychosocial effects of cooccurring disorders i the recovery process for cooccurring disorders i Medications to treat cooccurring disorders, their side effects, and medication management i Coping with cravings, anger, anxiety, boredom, and depression i Changing negative or maladaptive thinking i Developing a sober support system i Addressing family issues i Learning to use leisure time constructively i Spirituality in recovery i Joining 12Step and cooccurring disorder recovery mutualhelp groups i Risk factors in ongoing recovery i Understanding and getting maximum benefits from psychotherapy and counseling Adapted from Daley 2000. The psychiatric i All prescribed psychotropic medications medications should be, in most instances, should be to treat suspected or confirmed adjunctive to other ongoing interventions, not a cooccurring disorders, not to alleviate nor substitute for them. From a practical viewpoint and group, but all information should be commu assuming sufficient time to observe patients nicated both in writing and orally. Methadone withdrawal fluoxetine do not increase methadone levels symptoms may occur after discon (Prozacfi), significantly. Increase and/or split opioid withdrawal symptoms (Eap the methadone dosage to increase et al. Tricyclics Methadone impairs the metabolism Adjust doses of tricyclic desipramine, of tricyclics and can cause medications as needed; monitor increased tricyclic medication blood levels if clinically indicated. However, evidence sug example is a study of patients with chronic gests major differences in the abuse liability of depression who were treated with the tricyclic benzodiazepines. Fiftyseven percent of action such as oxazepam rarely are mentioned imipraminetreated patients showed both signifi as substances of abuse, have a wide margin of cant improvement in mood and some decreases safety, and are effective in reducing anxiety, in illicit drug use according to selfreports, com even over extended periods (Sellers et al. Sellers and colleagues also found a to presume that tricyclic medications are iserious pattern of nontherapeutic benzodi unique among antidepressants improving azepine use. Mood stabilizers shown to be effective include lithium, valproate, and the consensus panel believes that patients who carbamazepine (Hellewell 2002). Lamotrigine have a history of benzodiazepine abuse should (Lamictalfi) also has been shown to be effective. Some Patients sometimes respond better to one drug drugtesting laboratories can determine specific class or a specific drug in a class. If such a another antidepressant should be considered if resource is available, testing can determine patients do not respond to their first one after a whether patients are using only their prescribed 4 to 8week trial. Some antidepressants also benzodiazepines or supplementing them with have sedative effects. The latter would indi [Remeronfi], trazodone, and some tricyclic cate a need to change patientsi treatment plans. Nonsedating antidepressants Stimulants such as methylphenidate (Ritalinfi) might be especially useful for patients with are the treatment of choice for childhood psychomotor inhibition. However, they should be monitored carefully because some patients have abused Collaboration Betw een them by injection, and medical complications Counselors and Physicians can result from longterm injection use.
Conversely arthritis treatment knee pain generic trental 400 mg mastercard, among the ten states mostly likely to have mentally ill individuals in jails and prisons rheumatoid arthritis images cheap 400 mg trental with visa, five were also among the states spending the least money per capita arthritis healthy diet order cheapest trental. Another way to look at this problem is to ascertain what percentage of individuals with serious mental illnesses are put in jail i have arthritis in my fingers what can i do best trental 400 mg. The country has reverted to a situation last seen in the early 19th century arthritis diet daily mail buy trental cheap, when reformers such as Dorothea Dix inspired state legislatures to build psychiatric hospitals in which to place mentally ill individuals so that they would be treated more humanely arthritis fingers herbs order cheap trental. Problems Associated with Having Seriously Mentally Ill Persons in Jails and Prisons Jails and prisons are not created to be de facto mental hospitals. They are not structurally appropriate for patients, and the staffs are not recruited as psychiatric caretakers. Not surprisingly, there are many problems associated with placing large numbers of seriously mentally ill individuals into jails and prisons. Consequently the recidivism rate is thought to be higher than it is for other released prisoners. Also included was a 34yearold woman diagnosed with schizophrenia who had been charged with 12 felonies and 31 misdemeanors. At the Palm Beach County Jail, Jonathan Goode, diagnosed with schizoaffective disorder, was booked 49 times in 40 months between March 2006 and July 2009. The record for repeat offenders probably belongs to Gloria Rodgers, who after 259 arrests in Memphis, was finally committed to a state psychiatric hospital. Like many frequent flyers, Rodgers considered the Shelby County Jail to be her home. In Broward County, Florida, it costs $80 a day to house a regular inmate but $130 a day for an 9 inmate with mental illness. In Palm Beach County, each time Jonathan Goode was arrested he was required to have a psychiatric exam, each costing $2, 000, producing an expenditure of $98, 000 over 40 months. The main reason mentally ill inmates stay longer is that many find it difficult to understand and follow jail and prison rules. In one study, jail inmates were twice as likely (19 percent versus 9 percent) to be charged with facility rule violations. In another study in the Washington State prisons, mentally ill inmates accounted for 41 percent of infractions even though they constituted only 19 percent of the prison population. Another reason mentally ill inmates stay longer is that they are often held 41 for months awaiting the availability of a bed in a psychiatric hospital. Many of the correctional officers do not understand, and have little or no training in, how to work with mentally ill inmates. For the approximately half of discharged patients who have ended up homeless or in jails and prisons, it has been a personal tragedy. Although deinstitutionalization was well intentioned, the failure to provide for the treatment needs of the patients has turned this policy into one of the greatest social disasters of the 20th century. It is an ongoing disaster because states are continuing to close psychiatric hospital beds, with present administrators of state mental health programs seemingly oblivious to the problems they are causing. The present mental health system appears to be bankrupt of ideas for fixing this disaster. Marcy State Psychiatric Hospital was shut down many years ago and turned over to the State Department of Corrections to become the Marcy Correctional Facility. Then, in December 2009, it was announced that the Marcy Correctional Facility would open a 100bed Residential Mental Health Unit for inmates with serious mental illness. Thus, seriously mentally ill individuals who were once treated in the psychiatric hospital may end up being treated in exactly the same building, except that now it is called a prison. In less than 200 years, we have taken mentally ill individuals who were in jails and prisons; transferred them to mental hospitals; then we closed down the mental hospitals, thereby forcing the mentally ill individuals back to jails and prisons. This seems like a classic case study on how not to execute public administration, a neverending cycle of failed policies. The court thus becomes the de facto treating authority, a task originally assigned to the failed psychiatric outpatient clinics and community mental health centers. Then tie the federal mental health block grant to the results by state, with states having the fewest mentally ill prisoners getting the most money. States should also require that county departments of mental health pay the local corrections department for the treatment costs of all seriously mentally ill jail inmates. The present fiscal incentives encourage states to empty hospitals, even if the patients end up in jails or homeless; there are no fiscal incentives to follow up and make sure the patients receive care once they leave the hospitals. Many times, it is this very dangerousness standard that necessitates law enforcement involvement. Mentally ill individuals should be able to access treatment before they become dangerous or commit a crime, not after. Louis Dwight, a Congregationalist minister in Massachusetts, was shocked by what he saw when he began taking Bibles to prisoners in jails. Shortly thereafter the legislature approved the erection of the State 62 Lunatic Asylum at Worcester for 120 patients. Dorothea Dix, the most famous and successful psychiatric reformer in American history, picked up where Dwight left off. During 1841 and 1842, she visited every jail in Massachusetts and documented the mistreatment of mentally ill prisoners. Raise up the fallen; succor the desolate; restore the outcast; defend 63 the helpless. At the time Dix was advocating on behalf of mentally ill persons incarcerated in jails and prisons, there was approximately 1 public psychiatric bed available for every 5, 000 people in the population (the 1850 census, the first reliable enumeration of mentally ill persons in the United States, counted 4, 730 insane persons in the total population of 23, 261, 000). A century later, in 1955, prior to the beginning of deinstitutionalization of mental patients in the United States, there was approximately 1 public psychiatric hospital bed available for every 300 people in the population (559, 000 patients in state and county 64 mental hospitals in a total population of 165, 000, 000). During those 100 years, there were some changes in diagnostic nomenclature, but public psychiatric hospital beds were largely reserved for individuals with serious mental illnesses, specifically schizophrenia, schizoaffective disorder, bipolar disorder, and major depression. The advocacy efforts of Dorothea Dix and her colleagues to move mentally ill persons from jails and prisons to mental hospitals were largely successful. Other studies done between 1880 and 1960 also found comparatively low prevalence rates of mentally ill persons in jails and prisons. Thus, for almost 100 years, the problem of mentally ill persons in jails and prisons appeared to have been solved. These individuals were treated as patients, not as criminals, and were sent to mental hospitals, although the hospitals had little treatment to offer them at that time. He postulated that the two populations were inversely correlated: as one 67 decreases, the other increases. Paige Harrison and Margaret Noonan at the Bureau of Justice Statistics kindly guided us through the prisoner data. Faith Dickerson, who provided statistical assistance, and Judy Miller, who provided administrative assistance. Fuller Torrey, Nowhere To Go: the Tragic Odyssey of the Homeless Mentally Ill (New York: Harper and Row, 1988), chapters 3 and 4. Belcher, Are jails replacing the mental health system for the homeless mentally illfi Ditton, Mental health and treatment of inmates and probationers, Bureau of Justice Statistics Special Report, July 1999. Bichler 15 Robertson, Prevalence estimates of psychiatric disorders in correctional settings, the Health Status of Soon tobeReleased Inmates: A Report to Congress, April 2002, vol. Glaze, Mental health problems of prison and jail inmates, Bureau of Justice Statistics Special Report, September 2006, revised December 14, 2006. Elliott, Jailing mentally ill for minor offenses helps no one, Atlanta JournalConstitution, April 4, 2002; A. Gruver, Sedgwick County considers jail pod for mentally ill inmates, Wichita Eagle, April 30, 2009. Hermes, Boone County struggles to meet mental health care needs for inmates, Missourian, December 17, 2007. Michel, Jails struggle with a flood of mentally ill offenders, Buffalo News, July 22, 2002. Satija, Toledo area jails facing growing numbers of the mentally ill: inmate influx is attributed to fewer hospitals, Toledo Blade, August 30, 2009. Fields, No way out: trapped by rules, the mentally ill languish in prison, Wall Street Journal Online, May 3, 2006, online. Murray, Finding escape behind bars: when jail is the only place mentally ill inmates get treatment, they come back, and it costs $87 million, Houston Chronicle, July 21, 2008. The prison data are based on the National Prison Statistics obtained annually from each state. The jail data are based on the 2005 Census of Jail Inmates, a survey done approximately every five years. Six states (Alaska, Connecticut, Delaware, Hawaii, Rhode Island, and Vermont) operate joint prison and jail systems. Kleinberg, System at loss for solutions to multipletime, smalltime offenders, Palm Beach Post, January 31, 2010; S. Hammack, Jail can offer temporary refuge for those suffering from mental illness, Roanoke Times, October 15, 2007. Bender, Community treatment more humane, reduces criminaljustice costs, Psychiatric News 2003;38:28; A. Turner, Ethical issues in criminal justice administration, American Jails, January/February 2007; F. Butterfield, Study finds hundreds of thousands of inmates mentally ill, New York Times, October 22, 2003. Casella, Locking down the mentally ill, the Real Cost of Prisons Weblog, February 24, 2010, realcostofprisons. Johnson, Jail suicides reach record pace in state, Los Angeles Times, June 16, 2002. McKee, Lack of mentalhealth treatment options clogs criminal justice system, Helena Independent Record, October 2, 2007.
Digital tion rheumatoid arthritis nails order trental paypal, the boy has only one palpable testis in rectal examination reveals an enlarged the scrotum arthritis pain relief balm kingston chemicals 400 mg trental sale. Further examination reveals a prostate rheumatoid arthritis qigong buy trental uk, and the consistency is rubbery palpable mass in the left inguinal region arthritis in back at 30 years old order trental 400 mg mastercard. He (A) Alkaline phosphatase denies urinary frequency arthritis in the back with bone spurs cheap trental 400 mg without prescription, hesitancy rheumatoid arthritis diet indian purchase generic trental on line, or (B) Androgens dysuria. Imaging ofthe (E) Human chorionic gonadotropin spine suggests osteoblastic involvement of Answers and Explanations 1. Priapism is an intractable, often painful erection associated with condi tions such as sickle cell anemia, hypercoagulable states, spinal injuries, and some drugs. Balanitis is associated with poor hygiene and results from inflammation of the glans penis. Hypospadias is an anatomical anomaly wherein the urethral meatus opens on the ventral side ofthe penis. Chlamydia trachomatis is one ofthe leading causes ofurethritis and should be suspected whenever a gonorrhealike discharge fails to show gramnegative diplococci within neutrophilic phagocytes. Bowen disease presents as a single erythematous plaque on the penis or scrotum and may evolve into invasive carcinoma. Treponema pallidum causes syphilis, which may present with a painless chancre on the penis. Cryptorchidism (undescended testis) predisposes to testicular atrophy and sterility. It is associated with an increased incidence ofgerm cell tumors ofthe testis, even ifthe testis is surgically moved from its ectopic location back to the scrotum. A varicocele results from dilation ofthe veins of the spermatic cord, and the term "bag ofworms" aptly describes the abnormality. Serum human chorionic gonadotropin levels, elaborated by syncytiotrophoblasts, are elevated in about 15% ofcases, but these elevations are not as high as those seen in choriocarcinoma. Yolk sac tumor is the most common tumor ofthe testis during infancy and early childhood and is usually accompanied by an increase in serum afetoprotein. Endodermal sinus (yolk sac) tumor is the most common malignant germ cell tumor ofthe testis in infancy and early childhood. It is characterized by an increase in serum afetoprotein, aswell as histologically stainable aIantitrypsin. Choriocarcinoma is less common in this age group and often results in an increase in human chorionic gonadotropin. Leydig cell tumors are derived fromtesticular stroma and produce androgens and estrogens, often presenting with precocious puberty. Teratomas contain multiple germ layers and numerous tissues, including hair, teeth, and sebaceous tissue. It is derived from the conversion from testosterone by the action of the enzyme Sareductase, type 2. Pharmaceutical inhibition of this enzyme is useful in the medical management of benign prostatic hyperplasia. Human chorionic gonadotropin and afetoprotein are serum tumor markers for testicular cancers and bear no relevance to benign prostatic hyperplasia. Serum alkaline phosphatase is an indicator ofosteoblastic lesions in this advanced and unfortunate patient presentation. Both prostatespecific antigen and serum prostatic acid phosphatase are increased in prostatic cancer. Serum afetoprotein and serum human chorionic gonadotropin are elevated in various germ cell neoplasms ofthe testis. Vulvar dystrophies are a group of disorders of epithelial growth that often present with leukoplakia, a white, patchlike lesion. Leukoplakia can be a manifestation of several diverse processes and should be evaluated by biopsy. Bacterial vaginosis(Gardnerelavaginitis) is the most common cause ofvaginal discharge. Characteristically, it is a thin, homogeneous vaginal discharge with a malodorous, fishy amine odor, especially on addition of 10% potassium hydroxide. The cause is a loss of the normal vaginal lactobacilli, a consequent overgrowth of anaerobes. This type of vaginitis accounts for many cases formerly classified as nonspecific vaginitis. Bacterial vaginosis is associated with increased numbers of the facultative anaerobe Gardnerella vaginalis. It is caused by exotoxin produced by Staphylococcus aureus, which grows in the tampon. Characteristic features include fever, vomiting, and diarrhea, sometimes followed by renal failure and shock. It is characterized by purulent acute inflammation, initially of the urethra, paraurethral and Bartholin glands, and Skene ducts. Gonorrhea can result in extragenital infections, including: (1) Pharyngitis associated with orogenital sexual contact (2) Proctitis associated with anal intercourse (3) Purulent arthritis, which is most often monoarticular, involving a large joint, such as the knee, as a consequence ofbloodborne infection (4) Ophthalmia neonatorum, a neonatal conjunctival infection acquired at delivery 6. Multinucleated giant cells with viral inclusions are found in cytologic smears from lesions. The disease is sometimes manifest during secondary syphilis as condyloma lata, which are gray, flattened, wartlike lesions. Syphilis is a hazard during pregnancy because spirochetes can cross the placenta and result in fetal malformation. Chancroid is characterized by a soft and painful ulcerated lesion in contrast to the chancre of syphilis, which is firm and painless. An infection appears initially as a papule, which becomes superficially ulcerated. Squamous cell carcinoma is most often due to extension of squamous cell carcinoma of the cervix. Clear cell adenocarcinoma ofthe cervix and vaginal adenosis may also occur in these patients. Presenting features include multiple polypoid masses resembling a "bunch ofgrapes" projecting into the vagina, ofen protruding from the vulva. Cervical polyps are inflammatory proliferations of cervical mucosa; they are not true neoplasms. Disordered epithelial growth manifest by loss of polarity and nuclear hyerchromasia, beginning at the basal layer and extending outward, is characteristic. The cancer is most often squamous cell carcinoma; adenocarcinoma accounts for approximately 5% ofcases. It evolves through a series of increasing epithelial abnormalities proceeding from dysplasia to carcinoma in situ and then to invasive carcinoma. Since the introduction ofthe Papanicolaou (Pap) cytologic screening test, squamous cell carcinoma has exhibited a striking decrease in mortality. Early sexual activityand multiple sexual partners are associated withincreased incidence. Incidence ishigh in prostitutes, rare in celibates, and rare in some Jewish populations. The traditional belief that circumcision of male sexual partners exerts a protective effect has not been confirmed. Cigarette smoking is also associated with increased incidence, but the relationship remains unclear. Chronic specific (granulomatous) endometritis is most often tuberculous in etiology. The condition is characteristically responsive to hormonal variations of the menstrual cycle. Menstrualtype bleeding occursinto the ectopic endometrium, resulting in bloodfilled, or socalled "chocolate, " cysts. Endometriosis occurs most often in the pelvic area; the ovary is the most common site, followed by the uterine ligaments, rectovaginal septum, pelvic peritoneum, and other sites. It is sometimes a precursor lesion ofendometrial carcinoma; the riskofcarcinoma varies with the degree of cellular atypia. This is the most common uterine tumor and the most common ofall tumors inwomen; the incidence is increased in women ofAfrican lineage. They often increase in size during pregnancy, and they almost always decrease in size following menopause. It arises de novo and is almost never caused by malignant transformation ofa leiomyoma. Peak occurrence is in older women, who are affected more by endometrial carcinoma than by carcinoma ofthe cervix. The cancer is often preceded by endometrial hyperplasia, especially higher grade dysplasias. This disorder is most often associated with inflammation of the ovaries and other adjacent tissue (pelvic inflammatory disease). Salpingitis can result in pyosalpinx, a tube filled with pus, or hydrosalpinx, a tube filled with watery fluid; it mayalso result in a tuboovarian abscess. Adenocarcinoma most often results from direct extension or metastasis from tumors originating elsewhere. It is symptomatically associated with menstrual irregularity, occasionally with intraperitoneal hemorrhage. This cyst is a bloodcontaining cyst resulting from ovarian endometriosis with hemorrhage. Polycystic ovary syndrome may be associated with insulin resistance with an increased risk of diabetes mellitus. Morphologic characteristics include the following: (1) Markedly thickened ovarian capsule (2) Multiple small follicular cysts containing a granulosa cell layer and a luteinized theca interna (3) Cortical stromal fibrosis with islands offocal luteinization B. Tumors of surface epithelial origin make up almost three fourths of ovarian tumors.
Purchase generic trental line. Gout Diet Dos & Don'ts.