
J. W. Thomas Byrd, MD
- Nashville Sports Medicine Foundation, Nashville, Tennessee
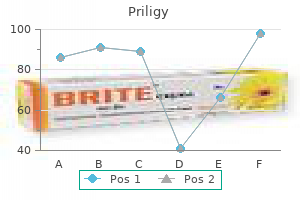
This parameter will correlate with the extent of chromasia exhibited by the stained cells and is calculated from the hemoglobin and hematocrit erectile dysfunction at age 17 order generic priligy line. This parameter is useful when evaluating erythrocyte morphology on a stained blood smear erectile dysfunction other names purchase priligy 30 mg on line. Megakaryocyte A large cell found within the bone marrow characterized by the presence of large or multiple nuclei and abundant cytoplasm relative impotence judiciary generic priligy 30mg. Megaloblastic Asynchronous maturation of any nucleated cell type characterized by delayed nuclear development in comparison to the cytoplasmic development erectile dysfunction question priligy 60mg with amex. The abnormal cells are large and are characteristically found in pernicious anemia or other megaloblastic anemia erectile dysfunction drugs dosage order 30 mg priligy amex. Microenvironment A unique environment in the bone marrow where orderly proliferation and differentiation of precursor cells take place impotence urology buy priligy 30 mg cheap. Mixed lineage acute An acute leukemia that has both myeloid and leukemia lymphoid populations present or blasts that possess myeloid and lymphoid markers on the same cell. The monoblast has nonspecific esterase activity that is inhibited by sodium fluoride. Monoclonal An alteration in immunoglobulin production that gammopathies is characterized by an increase in one specific class of immunoglobulin. Monocytemacrophage A collection of monocytes and macrophages, system found both intravascularly and extravascularly. Morulae Basophilic, irregularly shaped granular, cytoplasmic inclusions found in leukocytes in an infectious disease called ehrlichiosis. Mosaic Occurs in the embryo shortly after fertilization, resulting in congenital aberrations in some cells and some normal cells. The cell is associated with chronic plasmocyte hyperplasia, parasitic infection, and malignant tumors. Multiple myeloma Plasma cell malignancy characterized by increased plasma proteins. In instances where large sequences of nucleotides are missing, the alteration is referred to as a deletion. Myelofibrosis with A myeloproliferative disorder characterized by myeloid metaplasia excessive proliferation of all cell lines as well as progressive bone marrow fibrosis and blood cell production at sites other than the bone marrow, such as the liver and spleen. Myeloidtoerythroid ratioThe ratio of granulocytes and their precursors to (M:E ratio) nucleated erythroid precursors derived from performing a differential count on bone marrow nucleated hematopoietic cells. Myeloperoxidase An enzyme present in the primary granules of myeloid cells including neutrophils, eosinophils, and monocytes. Myelophthisis Replacement of normal hematopoietic tissue in bone marrow by fibrosis, leukemia, or metastatic cancer cells. National Committee for National agency that establishes laboratory Clinical Laboratory standards. Neutrophil A mature white blood cell with a segmented nucleus and granular cytoplasm. Seen in bacterial infections, inflammation, metabolic intoxication, drug intoxication, and tissue necrosis. Normal pooled plasma Plateletpoor plasma collected from at least 20 individuals for coagulation testing. The plasma is pooled and used in mixing studies to differentiate a circulating inhibitor from a factor deficiency. Nuclearcytoplasmic A condition in which the cellular nucleus matures asynchrony slower than the cytoplasm, suggesting a disturbance in coordination. As a result, the nucleus takes on the appearance of a nucleus associated with a younger cell than its cytoplasmic development indicates. This is usually estimated as the ratio of the diameter of the nucleus to the diameter of the cytoplasm. In immature hematopoietic cells the N:C ratio is usually greater than in more mature cells. It is not present in cells that are not synthesizing proteins or that are not in mitosis or meiosis. Nucleus (pl: nuclei) the characteristic structure in the eukaryocytic cell that contains chromosomes and nucleoli. In young, immature hematopoietic cells, the nuclear material is open and dispersed in a lacy pattern. As the cell becomes mature, the nuclear material condenses and appears structureless. Most oncogenes are altered forms of normal genes that function to regulate cell growth and differentiation. Optimal counting area Area of the blood smear where erythrocytes are just touching but not overlapping; used for morphologic evaluation and identification of cells. Vitamin K is required for the synthesis of functional prothrombin group coagulation factors. Orthochromatic A nucleated precursor of the erythrocyte that normoblast develops from the polychromatophilic normoblast. On romanowsky stain, visible near the periphery of the cell and often occur in clusters. PelgerHuet anomaly An inherited benign condition characterized by the presence of functionally normal neutrophils with a bilobed or round nucleus. Peripheral membrane Protein that is attached to the cell membrane by protein ionic or hydrogen bonds but is outside the lipid framework of the membrane. Petechiae Small, pinheadsized purple spots caused by blood escaping from capillaries into intact skin. Phagocytosis Cellular process of cells engulfing and destroying a foreign particle through active cell membrane invagination. Phagolysosome A digestive vacuole (secondary lysosome) formed by the fusion of lysosomes and a phagosome. Phase microscopy A type of light microscopy in which an annular diaphragm is placed below or in the substage condenser, and a phase shifting element is placed in the rear focal plane of the objective. This causes alterations in the phases of light rays and increases the contrast between the cell and its surroundings. Plasma cell A transformed, fully differentiated B lymphocyte normally found in the bone marrow and medullary cords of lymph nodes. May be seen in the circulation in certain infections and disorders associated with increased serum globulins. The cell is characterized by the presence of an eccentric nucleus containing condensed, deeply staining chromatin and deep basophilic cytoplasm. The large Golgi apparatus next to the nucleus does not stain, leaving an obvious clear paranuclear area. Plasmacytosis the presence of plasma cells in the peripheral blood or an excess of plasma cells in the bone marrow. Plasminogen A globulin, singlechain glycoprotein that circulates in the blood as a zymogen. Large amounts of plasminogen are absorbed with the fibrin mass during clot formation. Platelets play an important role in primary hemostasis adhering to the ruptured blood vessel wall and aggregating to form a platelet plug over the injured area. Platelet aggregation Platelettoplatelet interaction that results in a clumped mass; may occur in vitro or in vivo. Platelet procoagulant the property of platelets that enables activated activity coagulation factors and cofactors to adhere to the platelet surface during the formation of fibrin. Has the potential to selfrenew, proliferate, and differentiate into erythrocytic, myelocytic, monocytic, lymphocytic, and megakaryocytic blood cell lineages. Poikilocytosis A term used to describe the presence of variations in the shape of erythrocytes. If stained with new methylene blue, these cells would show reticulum and would be identified as reticulocytes. Polyclonal gammopathy An alteration in immunoglobulin production that is characterized by an increase in immunoglobulins of more than one class. Polymorphic variants Variant morphology of a portion of a chromosome that has no clinical consequence. Substituents occupy each of the eight peripheral positions on the four pyrrole rings. Portland hemoglobin An embryonic hemoglobin found in the yolk sac and detectable up to eight weeks gestation. Postmitotic pool Also called the maturationstorage pool; the neutrophils in the bone marrow that are not capable of mitosis. Primary aggregation the earliest association of platelets in an aggregate that is reversible. Primary fibrinolysis A clinical situation that occurs when there is a release of excessive quantities of plasminogen activators into the blood in the absence of fibrin clot formation. Excess plasmin degrades fibrinogen and the clotting factors, leading to a potentially dangerous hemorrhagic condition. Primary hemostasis the initial arrest of bleeding that occurs with blood vessel/platelet interaction. Primary thrombocytosis An increase in platelets that is not secondary to another condition. A probe is composed of a nucleotide sequence that is complementary to the sequence of interest and is therefore capable of hybridizing to that sequence. Procoagulant An inert precursor of a natural substance that is necessary for blood clotting or a property of anything that favors formation of a blood clot. Progenitor cell Parent or anscestor cells that differentiate into mature, functional cells. Prolymphocyte the immediate precursor cell of the lymphocyte; normally found in bone marrow. It is slightly smaller than the lymphoblast and has a lower nuclear to cytoplasmic ratio. Cytochemically, the cells stain positive for nonspecific esterase, peroxidase, acid phosphatase, and arylsulfatase. The distinguishing feature is the presence of large blueblack primary (azurophilic) granules. The granules contain acid phosphatase, myeloperoxidase, acid hydrolases, lysozyme, sulfated mucopolysaccharides, and other basic proteins. The cell is derived from the pluripotential stem cell and is found in the bone marrow. Prothrombinase complexA complex formed by coagulation factors Xa and V, calcium, and phospholipid. Prothrombin group the group of coagulation factors that are vitamin Kdependent for synthesis of their functional forms and that require calcium for binding to a phospholipid surface. This redistribution of cells accompanies vigorous exercise, epinephrine administration, anesthesia, convulsion, and anxiety states; also called immediate or shift neutrophilia. Unlike the real PelgerHuet anomaly, the nucleus of this cell contains a significant amount of euchromatin and stains more lightly. A critical differentiation point is that all neutrophils are equally affected in the genetic form of pelger huet anomaly, but only a fraction of neutrophils will be hyposegmented cells in the acquired state. Pulmonary embolism Obstruction of the pulmonary artery or one of its branches by a clot or foreign material that has been dislodged from another area by the blood current. Purging A technique by which undesirable cells that are present in the blood or bone marrow products are removed. Pyknotic Pertaining to degeneration of the nucleus of the cell in which the chromatin condenses to a solid, structureless mass and shrinks. These limits are used to determine if a test method is in control, and to minimize the chance of inaccurate patient results. If the test method is out of control, an intervention is required to reconcile the problem. Quiescence (G0) A phase in a cell that has exited the cell cycle and is in a nonproliferative state. R (relaxed) structure Conformational change in hemoglobin that occurs as the molecule takes up oxygen. Changes in the shape of the radar chart are indicative of different hematologic disorders. Random access Capability of an automated hematology instrument to process specimens independently of one another; may be programmed to run individual tests.
It is also necessary to work with men and boys beyond the field of sexual and reproductive health and rights diabetic erectile dysfunction pump order generic priligy. Engaging men economically in gender equality means promoting the sharing with women and girls of access to and control over agricultural resources b12 injections erectile dysfunction effective 90 mg priligy, opportunities for employment erectile dysfunction urinary tract infection purchase priligy online pills, and services erectile dysfunction louisville ky order on line priligy. There are also benefits for entire households when women participate equally in paid work erectile dysfunction doctor toronto cheap priligy 30 mg with amex. In short erectile dysfunction protocol foods to eat buy priligy master card, men in leadership positions can use their power to promote gender equality. These realities bring harm both to the lives of boys and men and to the lives of girls and women. On the positive side, there is evidence that younger generations of men in many parts of the world are more accepting of gender equality. While we can look at young men around the world and seek out their risktaking and harmful behaviors, we can also point to the young men who are already serving as voices and leaders for gender equality alongside young women. Framework of actions for follow up to the Programme of Action of the International Conference on Population and Development beyond 2014. A longitudinal and constructionist study of masculinity and the health risk behavior of young American men. Quantitative findings from the United Nations multicountry study on men and violence in Asia and the Pacific. The effect of power in sexual relationships on sexual and reproductive health: An examination of the evidence. Previniendo la violencia con jovenes: talleres con enfoque de genero y masculinidades. Gender dimensions of alcohol consumption and alcoholrelated problems in Latin America and the Caribbean. Dying to be men: Youth, masculinity and social exclusion (sexuality, culture and health). Guidelines for comprehensive sexuality education: Kindergarten through 12th grade. Global perspectives on the sexual and reproductive health of adolescents: Patterns, prevention and potential. Twenty years after International conference on population and development: Where are we with adolescent sexual and reproductive health and rightsfi Adolescent male sexuality and heterosexual masculinity: A conceptual model and review. Gender equitable boys in a gender inequitable world: Reflections from qualitative research and program development with young men in Rio de Janeiro, Brazil. Hidden violence: Preventing and responding to sexual exploitation and sexual abuse of adolescent boys briefing paper. Sexual abuse and exploitation of boys in South Asia: A review of research findings, legislation, policy and programme responses. I thought it could never happen to boys: Sexual abuse and exploitation of boys in Cambodia: an exploratory study. Gender relations, sexual violence and the effects of conflict on women and men in North Kivu, eastern Democratic Republic of Congo: Preliminary results of the International Men and Gender Equality Survey. Evolving men: Initial results from the International Men and Gender Equality Survey. Pathways to genderequitable men: Findings from the International Men and Gender Equality Survey in eight countries. Taking boys seriously: A longitudinal study of adolescent male schoollife experiences in Northern Ireland. United Kingdom: Department of Justice, Department of Education and the University of Ulster. School violence in South Africa: Results of the 2012 national school violence study. Schoolrelated genderbased violence is preventing the achievement of quality education for all: Policy paper 17. School bullying among adolescents in the United States: Physical, verbal, relational, and cyber. Parents, siblings and peer influences on adolescent substance abuse and alcohol problems. Alcohol, gender and drinking problems: perspectives from low and middle income countries. National poll reveals a disconnect between parents and teens on the role that social networking plays in their lives. The aim framework: Addressing and involving men and boys to promote gender equality and end gender discrimination and violence. International technical guidance on sexuality education: An evidenceinformed approach for schools, teachers and health educations. Bringing together knowledge, practice and alliances: A case study of a teacher training program on gender and sexuality in Brazil. A systematic review of interventions and a discussion of prevention of the risks of future violent behaviors of young boys. Program P: A manual for engaging men in fatherhood, caregiving, maternal and child health. Global and regional estimates of violence against women: Prevalence and health effects of intimate partner violence and nonpartner sexual violence. Synchronizing Gender Strategies: A cooperative model for improving reproductive health and transforming gender relations. Readers should be cognizant that new evidence may emerge following the publication of this report that could potentially influence the results. Patients may become severely visually impaired during childhood, adolescence, or early adulthood. Analytic Framework the analytic framework for this assessment is depicted in ure 1. This included correction of refractive error, low vision aids, and optimal access to educational and workrelated opportunities. Discussions with patient groups highlighted certain outcomes that we assessed as the evidence allowed. These included improvements in visual acuity, improvements in night vision, and a halting or slowing of disease progression. Timing Evidence on intervention effectiveness and harms were derived from studies of any duration. Clinical diagnosis is difficult and, when compared with genetic testing, has been found to incorrectly distinguish among individuals with the same mutation and categorize individuals with distinct mutations into similar phenotypes ure 2. Genetic testing is appropriate for most patients with presumed genetically caused retinal degeneration. It accounts for around 5% of all inherited retinopathies and is present in approximately 20% of children attending schools for the blind. Visual Cycle13 Gene Therapy Gene therapies modify the expression of genes to treat disease. These can involve strategies that repair genes or that introduce new genes into cells. The process of deliberately introducing functioning genes into cells is called transfection and is accomplished by using a vector, usually a virus. This does not repair or eliminate the defective gene, but rather introduces a normal copy of the gene into the cell. The retinabrain barrier limits the distribution of the vector into other organs and creates an immune privileged space limiting classical immune response, diminishing safety concerns about immune responses. In order to access the retina during the procedure, it is necessary to completely remove the vitreous gel that fills the eye, a process called vitrectomy. Cataracts are the most common complication, but infections and tears of the retina may also occur. The subretinal injection is administered into or near the macula, the area of the retina needed for visual acuity, and can lead to macular holes and tears and to infection. This spacing was designed to monitor for complications and reduce potential immune response from two administrations in a short timeframe. It is important to consider the possibility of degenerative processes continuing despite an improvement in photoreceptor functioning. Indeed, the mechanisms responsible for these degenerative processes that are leading to the final stage of the disease, the absence of light perception, are not well understood. As these mutant proteins are believed to contribute to retinal degeneration by different cytotoxic effects, 13, 23, 24 it is possible that degeneration continues, in spite of continuing therapeutic effect of the gene therapy. Neuroprotective therapies are currently being studied, and it has been proposed to eventually use them synergistically with gene therapy. A trial of stem cell treatments for various retinal degenerative diseases was started in 2016 and is expected to run until 2021. A treatment that delays the onset of visual impairment needs to be considered not simply in the number of years that visual loss is delayed, but also in terms of life stages. Completing education and entering the work force is another important life stage where delaying visual loss can potentially have important affects on easing transitions that are required when first becoming employed. Progressive vision loss can both create uncertainty for patients and require repeated readaptation of skills. We heard from patients that a therapy that stops decline in vision would be very important even if it did not improve vision. Such a therapy would provide greater certainty in decision making for the future base on stable skills and abilities. Patients and patient advocacy organizations emphasized the challenges of growing up with low vision both for affected children and their parents/families. Substantial adjustments are necessary for children to be able to perform at the same level as their peers in school, and their academic and career success may directly depend on the quality of assistive services and resources at their disposal. Because these services are, many times, provided outside of the health care system, traditional coverage policies do not address the needs of visually impaired individuals. For example, while Medicare does cover some rehabilitative services, other supportive services, like white canes or guide dogs, are not covered by private or public payers. In order to address these gaps in services, statelevel agencies, national organizations, and local organizations have created different programming designed to support individuals with low vision or blindness, so as to provide services and supports not provided by the healthcare system. We limited each search to Englishlanguage studies of human subjects and excluded articles indexed as guidelines, letters, editorials, narrative reviews, case reports, or news items. Further details of the search algorithms, methods for study selection, and data extraction are available in Appendix A and Appendix D. Study Selection We included evidence from all relevant clinical studies, irrespective of whether they used a comparative study design. We excluded abstracts that reported data also available in peerreviewed publications. Where data was only available from a press release, we did not include the information in our review. Data Extraction and Quality Assessment Data were extracted by one member of the research team and validated by two others. Because only one study was a randomized controlled trial, the overall quality of the supporting evidence was moderate. Attempts were made to negotiate with the sponsor to gain insight into endpoints that were missing or unclear.
Eating erectile dysfunction and marijuana generic 60mg priligy, drinking erectile dysfunction pills cost 30 mg priligy, smoking erectile dysfunction and diabetes a study in primary care buy priligy mastercard, handling contact lenses impotence from priapism surgery purchase priligy visa, applying cosmetics impotence nerve damage purchase 60mg priligy with mastercard, and storing food for human consumption must not be permitted in laboratory areas erectile dysfunction drugs and hearing loss purchase discount priligy online. Use of needles and syringes or other sharp instruments should be restricted in the laboratory, except when there is no practical alternative. Used needles must not be bent, sheared, broken, recapped, removed from disposable syringes, or otherwise manipulated by hand before disposal or decontamination. Used disposable needles must be carefully placed in punctureresistant containers used for sharps disposal, located as close to the point of use as possible. Decontaminate work surfaces with appropriate disinfectant after completion of work and after any spill or splash of potentially infectious material. Decontaminate all wastes before removal from the laboratory by an effective and validated method. Therefore, all laboratory personnel and particularly women of childbearing age should be provided with information 46 Biosafety in Microbiological and Biomedical Laboratories regarding immune competence and conditions that may predispose them to infection. All persons entering the laboratory must be advised of the potential hazards and meet specifc entry requirements in accordance with institutional policies. Only persons whose presence in the facility or individual laboratory rooms is required for scientifc or support purposes are authorized to enter. A logbook, or other means of documenting the date and time of all persons entering and leaving the laboratory must be maintained. All persons entering the laboratory must use laboratory clothing, including undergarments, pants, shirts, jumpsuits, shoes, and gloves (as appropriate). Used laboratory clothing must not be removed from the inner change room through the personal shower. These items must be treated as contaminated materials and decontaminated before laundering. After the laboratory has been completely decontaminated and all infectious agents are secured, necessary staff may enter and exit without following the clothing change and shower requirements described above. Laboratory personnel and support staff must be provided appropriate occupational medical services including medical surveillance and available immunizations for agents handled or potentially present in the laboratory. A system must be established for reporting and documenting laboratory accidents, exposures, employee absenteeism and for the medical surveillance of potential laboratoryassociated illnesses. The laboratory supervisor is responsible for ensuring that laboratory personnel: a. Receive appropriate training in the practices and operations specifc to the laboratory facility. Receive annual updates and additional training when procedural or policy changes occur. Removal of biological materials that are to remain in a viable or intact state from the laboratory must be transferred to a nonbreakable, sealed primary container and then enclosed in a nonbreakable, sealed secondary container. Laboratory equipment musts be routinely decontaminated, as well as after spills, splashes, or other potential contamination. Spills involving infectious materials must be contained, decontaminated, and cleaned up by appropriate professional staff, or others properly trained and equipped to work with infectious material. Equipment must be decontaminated using an effective and validated method before repair, maintenance, or removal from the laboratory. Equipment or material that might be damaged by high temperatures or steam must be decontaminated using an effective and validated procedure such as a gaseous or vapor method in an airlock or chamber designed for this purpose. All incidents must be reported to the laboratory supervisor, institutional management and appropriate 48 Biosafety in Microbiological and Biomedical Laboratories laboratory personnel as defned in the laboratory biosafety manual. Animals and plants not associated with the work being performed must not be permitted in the laboratory. After securing the outer doors, personnel within the laboratory retrieve the materials by opening the interior doors of the autoclave, fumigation chamber, or airlock. The doors of the autoclave or fumigation chamber are interlocked in a manner that prevents opening of the outer door unless the autoclave or fumigation chamber has been operated through a decontamination cycle. All equipment and supplies taken inside the laboratory must be decontaminated before removal from the laboratory. Daily inspections of essential containment and life support systems must be completed and documented before laboratory work is initiated to ensure that the laboratory is operating according to established parameters. These protocols must include plans for medical emergencies, facility malfunctions, fres, escape of animals within the laboratory, and other potential emergencies. Training in emergency response procedures must be provided to emergency response personnel and other responsible staff according to institutional policies. Safety Equipment (Primary Barriers and Personal Protective Equipment) Cabinet Laboratory 1. There must be gas tight dampers on the supply and exhaust ducts of the cabinet to permit gas or vapor decontamination of the unit. The cabinet should be designed to permit maintenance and repairs of cabinet mechanical systems (refrigeration, incubators, centrifuges, etc. Such materials should be centrifuged inside the cabinet using sealed rotor heads or centrifuge safety cups. Workers in the laboratory must wear protective laboratory clothing with a solidfront, such as tieback or wraparound gowns, scrub suits, or coveralls. No personal clothing, jewelry, or other items except eyeglasses should be taken past the personal shower area. All protective clothing must be removed in the dirty side change room before showering. Reusable clothing must be autoclaved prior to removal from the laboratory for laundering. Eye, face and respiratory protection should be used in rooms containing infected animals as determined by the risk assessment. Prescription eyeglasses must be decontaminated before removal through the personal body shower. Disposable gloves must be worn underneath cabinet gloves to protect the worker from exposure should a break or tear occur in a cabinet glove. All procedures must be conducted by personnel wearing a onepiece positive pressure supplied air suit. Workers must wear laboratory clothing, such as scrub suits, before entering the room used for donning positive pressure suits. All laboratory clothing must be removed in the dirty side change room before entering the personal shower. Inner disposable gloves must be worn to protect against break or tears in the outer suit gloves. Inner gloves must be removed and discarded in the inner change room prior to entering the personal shower. Decontamination of outer suit gloves is performed during laboratory operations to remove gross contamination and minimize further contamination of the laboratory. A doubledoor autoclave, dunk tank, fumigation chamber, or ventilated airlock must be provided at the containment barrier for the passage of materials, supplies, or equipment. A handsfree sink must be provided near the door of the cabinet room(s) and the inner change room. The internal surfaces of this shell must be resistant to chemicals used for cleaning and decontamination of the area. All penetrations in the internal shell of the laboratory and inner change room must be sealed. Openings around doors into the cabinet room and inner change room must be minimized and capable of being sealed to facilitate decontamination. Drains in the laboratory foor (if present) must be connected directly to the liquid waste decontamination system. Decontamination of the entire cabinet must be performed using a validated gaseous or vapor method when there have been signifcant changes in cabinet usage, before major renovations or maintenance shut downs, and in other situations, as determined by risk assessment. If, however, there is a central vacuum system, it must not serve areas outside the cabinet room. The supply and exhaust components of the ventilation system must be designed to maintain the laboratory at negative pressure to surrounding areas and provide differential pressure or directional airfow, as appropriate, between adjacent areas within the laboratory. A visual monitoring device must be installed near the clean change room so proper differential pressures within the laboratory may be verifed prior to entry. The air exhaust discharge must be located away from occupied spaces and building air intakes. Pass through dunk tanks, fumigation chambers, or equivalent decontamination methods must be provided so that materials and equipment that cannot be decontaminated in the autoclave can be safely removed from the cabinet room(s). Biological validation must be performed annually or more often if required by institutional policy. Effuents from showers and toilets may be discharged to the sanitary sewer without treatment. Autoclaves that open outside of the laboratory must be sealed to the interior wall. This bioseal must be durable and airtight and capable of 54 Biosafety in Microbiological and Biomedical Laboratories expansion and contraction. Rooms in the facility must be arranged to ensure exit by sequential passage through the chemical shower, inner (dirty) change room, personal shower, and outer (clean) changing area. The breathing air systems must have redundant compressors, failure alarms and emergency backup. A chemical shower must be provided to decontaminate the surface of the positive pressure suit before the worker leaves the laboratory. In the event of an emergency exit or failure of the chemical shower system, a method for decontaminating positive pressure suits, such as a gravity fed supply of chemical disinfectant, is needed. A doubledoor autoclave, dunk tank, or fumigation chamber must be provided at the containment barrier for the passage of materials, supplies, or equipment in or out of the laboratory. Sinks inside the suit laboratory should be placed near procedure areas and be connected to the wastewater decontamination system. Walls, foors, and ceilings of the laboratory must be constructed to form a sealed internal shell to facilitate fumigation and prohibit animal and insect intrusion. Drains, if present, in the laboratory foor must be connected directly to the liquid waste decontamination system. Services and plumbing that penetrate the laboratory walls, foors, or ceiling must be installed to ensure that no backfow from the laboratory occurs. Laboratory furniture must be of simple construction, capable of supporting anticipated loading and uses. Spaces between benches, cabinets, and equipment must be accessible for cleaning and decontamination. Chairs and other furniture must be covered with a nonporous material that can be easily decontaminated. An eyewash station must be readily available in the laboratory area for use during maintenance and repair activities. The supply and exhaust components of the ventilation system must be designed to maintain the laboratory at negative pressure to surrounding areas and provide differential pressure or directional airfow as appropriate between adjacent areas within the laboratory. Supply and exhaust fans must be interlocked to prevent positive pressurization of the laboratory. The ventilation system must be monitored and alarmed to indicate malfunction or deviation from design parameters. The exhaust air discharge must be located away from occupied spaces and air intakes. Biological safety cabinets can also be connected to the laboratory exhaust system by either a thimble (canopy) connection or a direct (hard) connection. Liquid effuents from chemical showers, sinks, foor drains, autoclave chambers, and other sources within the laboratory must be decontaminated by a proven method, preferably heat treatment, before being discharged to the sanitary sewer. Effuents from personal body showers and toilets may be discharged to the sanitary sewer without treatment. A doubledoor, pass through autoclave(s) must be provided for decontaminating materials passing out of the cabinet laboratory. When feasible, autoclave decontamination processes should be designed so that unfltered air or steam exposed to infectious material cannot be released to the environment. Provisions for emergency communication and emergency access or egress must be developed and implemented. In both instances, the institutional management must provide facilities, staff, and established practices that reasonably ensure appropriate levels of environmental quality, safety, security and care for the laboratory animal. As a general principle, the biosafety level (facilities, practices, and operational requirements) recommended for working with infectious agents in vivo and in vitro are comparable. In the animal room, the activities of the animals themselves can present unique hazards not found in standard microbiological laboratories. Animals may generate aerosols, they may bite and scratch, and they may be infected with a zoonotic agent. The coapplication of Biosafety Levels and the Animal Biosafety Levels are determined by a protocoldriven risk assessment. These recommendations presuppose that laboratory animal facilities, operational practices, and quality of animal care meet applicable standards and regulations. In addition, the organization must have an occupational health and safety program that addresses potential hazards associated with the conduct of laboratory animal research. Traffc fow that will minimize the risk of cross contamination should be incorporated into the facility design. The recommendations detailed below describe four combinations of practices, safety equipment, and facilities for experiments with animals involved in infectious disease research and other studies that may require containment. Investigators that are inexperienced in conducting these types of experiments should seek help in designing their experiments from individuals who are experienced in this special work.
Purchase priligy 90mg otc. Molo residents clash over erection of toilet near business premises.
Syndromes
- Limit foods that produce gas.
- Hematoma (blood accumulating under the skin)
- Dry AMD occurs when the blood vessels under the macula become thin and brittle. Small yellow deposits, called drusen, form. Almost all people with macular degeneration start with the dry form.
- What kind of shampoo, hair spray, gel, or other product do you put on your hair?
- Place catheters (tubes) around your heart to drain fluids that build up.
- Do you have any medical conditions, such as high blood pressure, diabetes, or high cholesterol?
This may be helpful in the diagnosis of dubious 341 Hematology cases of myelodysplasia erectile dysfunction medicine order genuine priligy, but the same abnormal pattern may be seen in nonclonal dysplastic states such as megaloblastic anemia erectile dysfunction and high blood pressure buy genuine priligy. Lam et al suggest the use of hexazotized pararosaniline as coupling reagent in a single incubation combined esterase erectile dysfunction drugs levitra order generic priligy pills, which gives contrasting bright red and brown reaction products erectile dysfunction foods to avoid safe priligy 60mg. Toluidine Blue Stain Toluidine blue staining is useful for the enumeration of basophiles and mast cells erectile dysfunction treatment centers cheap priligy online american express. It binds strongly to the granules in these cells erectile dysfunction natural treatment cheap priligy 90 mg without prescription, and is particularly useful in pathological states where the cells may not be easily 342 Hematology identifiable on Romanowsky stains. Interpretation of the result the granules of basophils and mast cells stain a bright red/purple, and are discrete and distinct. Although toluidine blue is said to be specific for these granules, with >10 min incubations, the primary granules of promyelocytes are stained red/ purple. However, these are smaller and finer than the mast cell or basophil granules an easily distinguished. Describe the importance of leucocyte cytochemistry in hematological investigation 3. Explain the interpretation of various leucocyte cytochemistry results: myeloperoxidase, Sudan black B, neutrophil alkaline phosphatase, acid phosphates, periodic acidshiff reaction, esterases, toluidine blue stain. It is initiated by vascular injury and culminates in the formation of a firm plateletfibrin barrier that prevents the escape of blood from the damaged vessel. Vascular damage exposes subendothelial structures to flowing blood, and blood platelets adhere and aggregate on the injured site. Simultaneously, coagulation proteins are sequentially activated to generate thrombin. Thrombin cleaves plasma fibrinogen into fibrin monomers, and thus polymerize to form a fibrin mesh over the adherent, aggregated platelets. Platelet contractile activity then draws the attached fibrin polymers more tightly over the injured vascular surface and away from the luminal blood flow. Plasmin, the active fibrinolytic enzyme generated on fibrin polymers, subsequently hydrolyzes the fibrin to soluble fragments. Properly constructed and metabolically intact vascular wall components, adequate numbers of functional platelets, and sufficient quantities of coagulation proteins are all necessary for normal hemostatsis. These multimers are composed of 230000 dalton monomers covalently linked by disulfide bonds into structures with molecular weights in the millions of daltons. Prostaglandin I2 is synthesized from the arachidonic acid that membrane lipases liberate from endothelial cell membrane phospholipids. Plasma coagulation factors are adsorbed onto their surface membranes and several are present in platelet granules. Thrombin, generated by the activation of the coagulation cascade, amplifies platelet aggregation and release responses. Platelet adherence to collage, as well as thrombininduce aggregation, causes a change in platelet membrane structure. Collage and thrombin activate platelet membrane lipases, which then hydrolyze arachidonic acid from ester bonds in platelet membrane phospholipids. Thromboxane A2, a shortlived prostaglandin derivative, potentiates the release of platelet granule contents. Any thromboxane A2 that leaks from activated platelets also induces other platelets to aggregate, and stimulates local vasoconstriction. It is hydrolyzed rapidly and nonenzymatically into an inactive end 351 Hematology product, thromboxane B2. Roman numerals are not used for prekallikrein and high molecular weight kininogen. In the final common pathway of the coagulation cascade, thrombin converts soluble, circulating fibrinogen into insoluble fibrin polymers. Thrombin 352 Hematology generation occurs through two different reaction sequences, the intrinsic and extrinsic coagulation pathways. Factor X also binds to membranes by calcium brides between carboxyglutamic acid residues in X and surface phospholipids. Following the activation of X to Xa, Xa remains plateletbound and attaches to activated factor V molecules (Va). Factor V is either adsorbed from plasma and then cleaved and activated to Va by thrombin, or released in Va form from platelet granules. One portion contains all the carboxyglutamic acid residues and may remain bound transiently to the platelets through calcium bridges. This protein is normally found on fibroblasts, but can also be expressed by white blood cells, smooth muscle cells, and endothelial cells in some situations. Normally, the extrinsic and intrinsic pathways are complementary mechanisms and both are essential for the formation of adequate amounts of factor Xa and thrombin in vivo. These mechanisms include neutralization within the blood of the enzymes and activated cofactors of coagulation and clearance of activated clotting factors, especially during hepatic circulation. Thrombin, when bound to a receptor on endothelial cells called thrombomodulin, can cleave a small peptide from and thus activate protein C. Factor V Leiden is a genetic mutation (substitution of arginine with glutamine at position 506) that decreases degradation of factor Va by activated protein C. These clinical observations establish the physiologic importance of the protein C/protein S mechanism for regulating coagulation. By dissolving fibrin, this system helps keep open the lumen of an injured blood vessel. A balance between fibrin deposition and lysis maintains and remolds the hemostatic seal during repair of an injured vessel wall. Plasmin arises from an inert plasma precursor, plasminogen, through cleavage of a single argininevaline peptide bond. Fibrin is first degraded into large 360 Hematology fragments (X and Y) and then into smaller fragments (D and E). When fibrinogen is converted to fibrin, lysine residues become available on the molecule to which plasminogen can bind tightly by way of lysinebinding sites. Two types of plasminogen activators triggering lysis of intravascularly deposited fibrin are released from vascular endothelial cells. The second type, urokinase, exists in singlechain and doublechain forms with different functional properties. A trace concentration of plasmin cleaves singlechain to doublechain urokinase plasminogen activator, which is an equally potent activator of plasminogen in solution and of plasminogen bound to fibrin. Epithelial cells that line excretory ducts (eg, renal tubules, mammary ducts) also secrete urokinase, which is thought to be the physiologic activator of fibrinolysis in these channels. Streptokinase, a bacterial product not normally found in 361 Hematology the body, is another potent plasminogen activator. The primary plasmin inhibitor is 2antiplasmin, which can very rapidly inactivate free plasmin escaping from a fibrin clot. Plasma also contains histidinerich glycoprotein, which is not a serine protease inhibitor but competes for lysinebinding sites on plasminogen, thus reducing the plasma concentration of plasminogen molecules with free lysinebinding sites. Moreover, plasmin escaping from the fibrin surface is almost instantaneously neutralized by 2 antiplasmin. Rarely, patients have an essentially total hereditary deficiency of 2antiplasmin. Their severe tissue bleeding after trivial injury establishes 2antiplasmin as a key regulator of normal fibrinolysis. An occasional patient with decompensated chronic liver disease may bleed uncontrollably because of excessive fibrinolysis thought to partially stem from acquired severe 2antiplasmin deficiency (secondary to diminished hepatocellular synthesis plus increased consumption caused by excessive plasminogen activator activity). Screening tests measure combined effects of factors that influence a particular phase of coagulation (eg, bleeding time). Additional tests may measure a product or effect of pathologic in vivo activation of platelets, coagulation, or fibrinolysis (eg, level of fibrin degradation products). Screening test results and knowledge of the clinical disorder guide the selection of more specific diagnostic tests. A disposable, springloaded bleeding time device is used to make a 6mm fi 1mm incision on the volar aspect of the forearm. Blood is absorbed onto the edge of a piece of filter paper at 30sec intervals until bleeding stops. Plasma is incubated for 3 min with a reagent supplying procoagulant phospholipid and a surfaceactive powder (eg, micronized silica). Because the test is independent of the reactions that generate thrombin, it is used to screen specifically for abnormalities affecting the thrombinfibrinogen reaction: heparin, large fibrin degradation products, and qualitative abnormalities of fibrinogen. It is particularly useful in establishing whether a plasma sample contains heparin (eg, residual heparin not neutralized after an extracorporeal bypass procedure or contaminated plasma obtained from blood drawn from a line kept open with heparin flushes). In plasma that contains heparin, the thrombin time will be prolonged, but a repeat test will be normal if the reagent batroxobin (a snake venom enzyme insensitive to heparin that directly converts fibrinogen to fibrin) is substituted for thrombin. A normal result does not rule out a milder yet potentially 368 Hematology clinically significant abnormality of fibrinolysis (eg, a reduced plasma 2antiplasmin level in the 10 to 30% of normal range). A falsepositive result may be caused by difficulty with venipuncture or by inadequate anticoagulation of a blood sample. In the Ddimer test, undiluted test plasma and diluted test plasma as necessary are mixed with latex particles coated with monoclonal antibodies that react exclusively with derivatives of fibrin that contain Ddimer, which are formed when plasmin degrades crosslinked fibrin. The antibodies will not react with fibrinogen itself, which is why the test can be performed on plasma, nor with fibrinogen degradation products because these are not crosslinked. A euglobulin lysis time is also often part of screening if increased fibrinolytic activity is suspected. The euglobulin fraction, which is relatively free of inhibitors of fibrinolysis, is clotted with thrombin, and the time for the clot to dissolve is measured. Normal lysis is > 90 min; a shorter time indicates increased plasma plasminogen activator activity (eg, in some patients with advanced liver disease). A reduced plasma fibrinogen concentration, by yielding a smaller clot to be dissolved, may also result in a shorter time. Disorders of hemostasis Excessive bleeding may occur as a result of an abnormality of blood vessels, platelets, or coagulation factors. Vascular disorders In vascular bleeding disorders, tests of hemostasis are 370 Hematology usually normal. Purpura Simplex (Easy Bruising) the most common vascular bleeding disorder, manifested by increased bruising and representing increased vascular fragility. The platelet count and tests of platelet function, blood coagulation, and fibrinolysis are normal. No drug prevents the bruising; the patient is often advised to avoid aspirin and aspirincontaining drugs, but there is no evidence that bruising is related to their use. Senile Purpura A disorder affecting older patients, particularly those who have had excessive sun exposure, in whom dark purple ecchymoses, characteristically confined to the extensor surfaces of the hands and forearms, persist for a long time. Lesions slowly resolve over several days, leaving a brownish discoloration caused by deposits of hemosiderin; this discoloration may clear over weeks to months. The skin and subcutaneous tissue of the involved area often appear thinned and atrophic. Hereditary Hemorrhagic Telangiectasia (Rendu OslerWeber Disease) A hereditary disease of vascular malformation transmitted as an autosomal dominant trait affecting men and women. Diagnosis is made on physical examination by the discovery of characteristic small, redtoviolet telangiectatic lesions on the face, lips, oral and nasal mucosa, and tips of the fingers and toes. These fistulas may produce significant righttoleft shunts, which can result in dyspnea, fatigue, cyanosis, or polycythemia. However, the first sign of their presence may be a brain abscess, transient ischemic attack, or stroke, as a result of infected or noninfected emboli. Cerebral or spinal arteriovenous malformations occur in some families and may cause subarachnoid hemorrhage, seizures, or paraplegia. Laboratory studies are usually normal except for evidence of irondeficiency anemia in most patients. The disease primarily affects young children but may affect older children and adults. An acute respiratory infection precedes purpura in a high proportion of affected young children. Less commonly, a drug may be the inciting agent, and a drug history should always be obtained. Biopsy of an acute skin lesion reveals an aseptic vasculitis with fibrinoid necrosis of vessel walls and perivascular cuffing of vessels with polymorphonuclear leukocytes. Granular deposits of immunoglobulin reactive for IgA and of complement components may be seen on immunofluorescent study. Therefore, deposition of IgAcontaining immune complexes with consequent activation of complement is 374 Hematology thought to represent the pathogenetic mechanism for the vasculitis. The disease begins with the sudden appearance of a purpuric skin rash that typically involves the extensor surfaces of the feet, legs, and arms and a strip across the buttocks. The purpuric lesions may start as small areas of urticaria that become indurated and palpable. Most patients also have fever and polyarthralgia with associated periarticular tenderness and swelling of the ankles, knees, hips, wrists, and elbows. The disease usually remits after about 4 wk but often recurs at least once after a diseasefree interval of several weeks. In most patients, the disorder subsides without serious sequelae; however, some patients develop chronic renal failure.