
Christopher Ethan Cox, MD
- Associate Professor of Medicine

https://medicine.duke.edu/faculty/christopher-ethan-cox-md
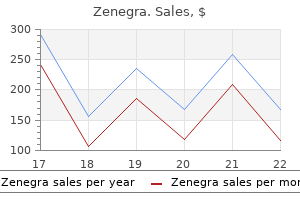
No diferences were observed across groups or between the blue and green target conditions on this task erectile dysfunction mayo clinic buy zenegra 100mg without prescription. As before impotence yahoo answers discount zenegra 100mg with amex, all participants were in structed to maintain their attention on the dot in the center of the screen until the rect angles appeared and then to shif their gaze to the target rectangle as quickly as possible erectile dysfunction surgery purchase 100 mg zenegra with visa. The logic was that if the woman had been covertly attending to the side of the screen with her own picture best male erectile dysfunction pills over the counter generic zenegra 100mg on-line, she would be able to respond more quickly when the target rectangle appeared on that side erectile dysfunction treatment orlando cheap zenegra 100 mg with visa. Moreover erectile dysfunction statistics singapore discount zenegra 100mg free shipping, when the target rectangle appeared on the opposite side from her own picture, she would fnd it harder to shif her gaze away from the covertly attended location, slow ing her response. On the other hand, if there is no attentional bias, then women should shif their gaze toward the target rectangle equally quickly regardless of where their own picture had appeared. Women who view their bodies very negatively may increase their attention to their appearance to maintain vigilance over a perceived threat to their self-worth. Perceptual and Cognitive Distortions Perceptual distortions and cognitive distortions are experiences and thoughts that do not correctly refect reality. Dichotomous thinking (also known as black and white thinking) is a cognitive dis tortion expressed in many of the features common to eating disorders. For example, individ uals with eating disorders may see thin as good and fat as bad. Conversely, foods such as celery, carrots, and diet sodas are low in calories and therefore good. For example, on a low-fat diet bacon is a bad food, and grapefruit is a good food. When individuals experience in creased stress, their ability to handle complex information diminishes (Vedhara, Hyde, Gilchrist, Tytherleigh, & Plummer, 2000). Similarly, bad foods are bad even when the social context and the initial portion size make consumption of those foods normal and desirable. Cognitive rigidity in individuals with eating disorders reveals itself as a perseverative approach to problems. As they lose more and more weight, however, they tend to become more depressed and more terrifed of weight gain. T us pa tients with eating disorders can engage in behaviors motivated to achieve a specifc end, only to fnd that the opposite result occurs. However, these individuals do not re-evaluate the usefulness of their behaviors according to the consequences; they simply persist in believing that they just havent done enough or just havent done it right. She contemplated asking him to stop buying these foods, but she was afraid of having to explain why. He was able to eat a few cookies at a time, and as far as he knew, a package of cookies would last a month. However, when asked, Jean was able to acknowledge that before her weight loss diet, she had been able to have one dessert afer dinner at a restaurant and not lose control of her eating later. She had always thought that the reason she showed restraint in this situation was that the restaurant controlled how much food she got. However, she had to admit that the restaurant did not keep her from later going to a store and buying a package of cookies or a gallon of ice cream. So she had, at one time in her life, been able to eat dessert without losing control. Although she has been able to eat just one dessert, she has convinced herself that she cant do so when she is alone. T erefore her only choices are to eat nothing or eat everything (a case of dichotomous thinking). As a short-term approach to losing weight, abstinence from forbidden foods may yield some success, because it may be easier to avoid some foods altogether than to eat a small amount of those foods. Beyond the potential for dieting to trigger physiological weight-defending mechanisms that contribute to binge eating (see the discussion of Keys et al. Indeed, would it even be possible to experience a loss of control over eating if one werent attempting to control eating in the frst place Polivy and Herman (1985) proposed that cognitive regulation of dietary intake (eating in response to rules about when to eat and what to eat rather than eating in re sponse to hunger) introduces opportunities for loss of control over eating (disinhibition). Disinhibition could occur in response to a cognitive trigger, an afective trigger, or a phar macological trigger. Afer having the cake, dieters might think that they have blown their diets and might as well eat whatever they want for the rest of the evening. An example of an afective disin hibitor is a fght with a loved one that leads to frustration and sadness. In this case, one may use cognitive resources normally employed to restrict food intake to cope with distress. In addition, one may use eating as a source of comfort and justify it as a special treat. An ex ample of a pharmacological disinhibitor is becoming intoxicated and losing track of what or how much one has eaten. Polivy and Herman (1985) argued that individuals who become chronic diet ers, or restrained eaters, lose the ability to determine when they feel hungry or full. When she is alone in the apartment and eats a cookie, she has failed and there is no reason for her to stop eating. In addition, her dieting has disrupted her ability to eat in response to hunger and stop eating in response to satiation. A series of experimental studies have demonstrated the infuence of dieting-related cognitions on food intake. In the classic study of this phenomenon, Spencer and Fremouw (1979) divided participants into restrained eaters and unrestrained eaters based on scores on a self-report measure of dietary restraint. Participants were then brought into a laboratory for a taste test (see Chapter 4 for a description of the basic taste-test study design). In the other condition, they were led to believe they were consuming a high-calorie milkshake. The milkshakes did not difer in actual nutri tional content, so there would be no physiological diferences in satiation. During the taste test, restrained eaters consumed signifcantly more in the high calorie than in the low calorie condition. Further, rather than compensat ing for the high-calorie shake by eating less (which would help them adhere more closely to their diets), restrained eaters ate more. Another cognitive phenomenon relevant to eating disorders is selective abstraction. Selective abstraction occurs when a part comes to represent the whole (Beck, 1970). For example, Emily was able to acknowledge that several areas of her body were not fat. However, she perceived fat on her thighs, and this one region caused her to evaluate her whole body as being in danger of becoming fat. Selective abstraction is particularly likely among perfectionists, because if something would be perfect if not for one specifc faw, then that one faw carries undue importance in evaluating the worth of the whole. In this task partici pants are asked to copy an abstract fgure with several detailed features onto a blank sheet of paper. Observations of how they approach this task suggest that when the fgure is present they achieve great accuracy in copying by going from detail to detail but never incorporate the overall shape of the image or how the parts ft together in a whole (Lopez et al. Putting this information together with that from previous chapters, societal messages that contribute to disordered eating, such as images that convey the importance of being thin, may be particularly salient to individuals who develop eating disorders. In addition, the ways that individuals use and evaluate that information likely contribute to disordered eating. Rather than feeling good about successes, whether large or small, people with eating disorders have cognitive distortions that leave them vulnerable to sufering innumerable perceived failures with respect to their eating, their bodies, and their lives. For adolescents, controlling weight and shape may seem like a manageable way to alleviate distress; however, for many, it becomes a trap. The few successes and numerous failures to control body weight and shape then negatively 117 PsyChologiCal faCtors 117 infuence self-evaluation and lead to increased eforts to alleviate distress through weight control (Heatherton & Baumeister, 1991). One limitation in this line of reasoning is that the cognitive features characteristic of eating disorders may not have predated the onset of an eating disorder. Instead they may refect an aspect or even a consequence of having an eating disorder. Research that suggests cognitive diferences from healthy controls in women recovered from eating disorders ofers some support for the idea that these thought processes predated and contributed to the onset of the eating disorder. A consequence of having an eating disorder could remain afer the eating disorder is in remission, much as a scar remains afer a wound has healed. Conclusion Research has revealed a high degree of overlap across aspects of personality, learning, and perceptual and cognitive distortions associated with the development of eating disorders. This overlap may be explained by the role of personality in shaping how individuals perceive, react to , and interact with their environments. T us an individual who is highly perfection istic and constrained and who demonstrates high persistence and harm avoidance may show a cognitive style marked by rigidity, dichotomous thinking, and selective abstraction that makes it difcult to make decisions that balance positive and negative consequences. This person would be more vulnerable to social messages conveying the importance of being thin. He or she also may be more likely to persist in the pursuit of this ideal even when the rewards diminish in intensity and the costs increase. Conversely, an individual who is impulsive may experience cognitive disinhibition more readily than others do. This person might fnd it more difcult to resist the rewarding aspects of food and eating. In combination with higher reward and punishment sensitivity, such a personality may contribute to a vicious cycle of binge eating and purging. These patterns provide a fairly coherent explanation of symptom atic diferences across eating disorders described in Chapter 1. Disordered eating symptoms may serve as a maladaptive solution to problems that elicit in tense negative emotional states. The failure to recognize that the symptoms do not actually solve the problem may result from a combination of cognitive distortions and the greater salience of immediate and perceived consequences than of long-term actual consequences. T us negative emotionality may be a common factor that bridges the diferent types of eating disorders. Key Terms Afective disinhibitor Central coherence Cognitive disinhibitor Cognitive distortions 118 118 eating DisorDers Constraint Dichotomous thinking Harm avoidance Negative emotionality Negative reinforcement Novelty seeking Operant conditioning Persistence Personality Pharmacological disinhibitor Positive emotionality Positive reinforcement Punishment Reward dependence Selective abstraction Temperament 119 8 Biological Bases, Correlates, and Consequences of Eating Disorders Research has revealed a variety of biological diferences between individuals with eating dis orders and those without eating disorders. Biological diferences may represent risk factors that were present before the onset of eating disorders. However, just as eating disorders afect psychological function, they afect biological functions, and biological diferences may re fect consequences of eating disorders. As discussed in Chapter 4, it would be unethical to directly test factors believed to cause eating disorders in humans by experimentally manipu lating those factors to see if they really did cause a disorder. Much of the biological research on eating disorders therefore cannot disentangle causes from consequences. T us this chap ter reviews biological bases, correlates, and consequences of eating disorders together. The frst section of this chapter reviews the biological bases of appetite and weight regulation and reward systems in the brain, as well as associations between the functions of diferent neurochemicals that impact these systems and eating disorders. This review reveals how the brain infuences hunger and satiation based on experimental studies in animals. However, it would be equally unwise to completely discount the role of such mechanisms in the etiology or maintenance of eating disorders. The second section of this chapter discusses the contribution of genes to the etiology of eating disorders. The section begins with an examination of data from behavioral genetic studies of families, twins, and adopted versus biological siblings. Because eating is a basic biological function required to sustain life, disruption of eating has profound efects 120 120 eating DisorDers on biological systems throughout the body. This fact explains the ambiguity associated with interpreting results from studies that attempt to reveal the biological bases of eating disor ders by examining individuals currently sufering from these disorders. Brain Function and Eating Disorders Appetite and Weight Regulation The hypothalamus (Figure 8. It can be divided into diferent sections named for their locations in relation to each other (Figures 8. Surgically damaging the ventromedial hypothalamus in animals produces increased food intake and signifcant obesity (Hetherington & Ranson, 1942). In contrast, surgically damaging the lateral hypothalamus produces dramatic de creases in food intake and weight loss (Anand & Brobeck, 1951; Teitelbaum & Stellar, 1954). Electrical stimulation of these brain regions produces the opposite efects (Kandel, Schwartz, & Jessell, 1991). These results suggest that the ventromedial hypothalamus is responsible for inhibiting appetite and food intake and that the lateral hypothalamus is responsible for increasing appetite and food intake. In healthy individuals these areas appear to work together to maintain a balance in weight and appetite. They are thought to be important in understanding satiety function as it may relate to eating pathology. In addition to regulating eating, the hypothalamus regulates body functions such as sexual activity, circadian rhythm, thermal regulation, and fuid balance. Medial view showing the relationship of the hypothalamus to the pituitary and thalamus. Neurotransmitters and Eating Disorders Neurotransmitters are chemicals that facilitate communication between brain cells (neu rons).
In the cat colon perfused with 10mM mesalazine erectile dysfunction medicine reviews order zenegra on line, the interstitial concentration of the drug was estimated as 130 M (20mg/l; Grisham and Granger erectile dysfunction age 60 100 mg zenegra with visa, 1989) erectile dysfunction treatment penile implants buy zenegra 100 mg cheap, sufficient for it to act erectile dysfunction blue pill purchase zenegra with paypal, as described below erectile dysfunction treatment non prescription cheap 100 mg zenegra mastercard, as a scavenger of free radicals erectile dysfunction pills for heart patients buy discount zenegra 100 mg online. Of the pro-drugs of mesalazine, the most widely used is sulphasalazine, which is poorly absorbed from the small intestine but metabolised in the large intestine to sulphapyridine and mesalazine. The released sulphapyridine is almost totally absorbed, in contrast to the poor absorption of mesalazine (Bondesen et al. The cleavage of sulphasalazine in the large intestine means that there is a delay of about 4 hours before any mesalazine or sulfapyridine is absorbed. This delay before the detection of sulphapyridine in blood has, in fact, been used as a test for the transit time to the large intestine (Kennedy et al. Of more clinical importance is that much of the haematological toxicity of sul phasalazine is due to the metabolite sulphapyridine (Pirmohamed et al. Olsalazine is, like sul phasalazine absorbed poorly from the small intestine (Sandberg-Gertzen et al. At least 30 per cent of an oral dose is absorbed as mesalazine and its metabolites (Willoughby et al. The conversion of the two pro-drugs to mesalazine and the subsequent absorption of the active form is very similar (Stretch et al. Comparison between the coated tablets and the pro-drugs is of interest in the therapeutic properties of mesalazine. In subjects with normal transit times, the presently available coated tablets release more mesalazine in the small intestine and less into the large intestine than the two pro-drugs (Rijk et al. For both the sustained release preparations and the pro-drugs, a decreased transit time through the gastrointestinal tract reduces the delivery of mesalazine to the large intestine, although the reduction is greatest for the two pro-drugs (Christensen et al. The formulation of these preparations has a marked effect on the spread and retention time in the colon, which are important factors in the effi cacy of the enemas (Otten et al. Rainsford Elimination Mesalazine is primarily eliminated by metabolism to N-acetyl-5-aminosalicylate (Figure 4. Mesalazine is not only acetylated systemically, presumably in the liver, but is also acetylated locally by intestinal ora (Dull et al. All are present in human plasma, but only trace amounts of the glucose conjugate are found in urine because of its instability under the pH conditions and temperature of urine. Like other aromatic amines mesalazine reacts non-enzymatically with glucose, but the amounts of the glucose conjugate in plasma are too great to be formed in this manner from the available concentrations of the drug and glucose. All the pathways of elimination have not yet been identi ed, and there are unidenti ed compounds in faeces and urine (van Hogezand et al. As is the case with salicylate, mesalazine is chemically modi ed by free radicals and the reactions may be related to its therapeutic activity in ulcerative colitis. Thus, faeces from such patients treated with sulphasalazine contain some of the same products that are produced by reaction of mesalazine with free radicals in the Fenton system (Ahnfelt-Ronne et al. These products are not present in faeces from rheumatoid patients treated with sulphasalazine, indicating that the local metabolism of mesalazine is speci c to ulcerative colitis. Mesalazine is metabolised by activated neutrophils and monocytes to yield salicylate and gentisate (Davis et al. Hypochlorous acid is formed by activated neutrophils, and several products have been identi ed or suggested from its reaction with mesalazine. Intermediates in the production of gentisate are the potentially toxic iminoquinone and quinone deriv atives, which react with thiols in a similar fashion to the reactive intermediate formed by the oxidation of paracetamol (Liu et al. Sul phasalazine, a diazo conjugate of mesalazine with sulphapyridine, is cleaved to yield mesalazine and sulphapyridine. Rainsford damaging effects of the activated cells in the in ammatory bowel disease, but could also decrease the antimicrobial activity of the white blood cells or lead to toxicity. A distributional phase with a half-life of 17 minutes is also seen when the drug is administered intravenously (Myers et al. Plasma concentrations of the acetyl metabolite are initially lower than those of mesalazine after intra venous dosage or after absorption from the upper gastrointestinal tract, but may exceed the lower plasma concentrations of unchanged mesalazine after release in the large intestine, consistent with the acetylation of the drug at this site. During long-term treatment with sulphasalazine, the plasma concen trations of the acetyl metabolite of mesalazine are markedly lower than after a single dose (Taggart et al. Although poorly absorbed, unchanged sulphasalazine and olsalazine are detectable in plasma after oral administration. During daily treatment with 2g sulphasalazine, the average concentrations of the unchanged drug are about 5mg/l (Taggart et al. The half-life of sulphasalazine in young patients with rheumatoid arthritis is about 6 hours, increasing to 10 to 20 hours in the elderly, although the plasma concentrations during long-term therapy in the elderly are not signi cantly higher than in young patients. Olsalazine has a shorter half-life of elimination, at about 55 minutes, while its sulphate conjugate has the surprisingly long half-life of about 7 days (Ryde and Ahnfelt, 1988). A method in which mesalazine and all the presently known metabolites are chromatographed appears to be very suitable for detailed pharmacokinetic studies (Tjornelund and Hansen, 1991). Absorption Di unisal is less water-soluble than either aspirin or salicylate, and its oral absorption is consequently slower (Nuernberg and Brune, 1989). Distribution Di unisal is bound to plasma albumin much more strongly than is salicylate. However, like salicylate, the unbound fraction of di unisal increases with the concentration of di unisal, and over the therapeu tic concentrations (50 to 250mg/l) the unbound fraction in human plasma nearly doubles from about 0. Like several strongly protein-bound drugs, the uptake into synovial uid is slow and lags behind the absorption of the drug (Nuernberg et al. Rainsford Elimination Di unisal is metabolised to acyl and phenolic glucuronides (Figure 4. Another difference is that the sulphate conjugate of di unisal accounts for about 10 per cent of the urinary metabolites in man (Loewen et al. A minor metabolite is 3-hydroxydi unisal, which is excreted as unidenti ed conju gate (Macdonald et al. As is the case with other acyl glucuronides, including that of salicylate, the acyl glucuronide of di u nisal is reactive. Three types of reactions occur; it is hydrolysed back to di unisal (see below), rearranged (Dickinson and King, 1989), and covalent adducts of di unisal are produced with proteins (Watt and Dickinson, 1990). The adducts with plasma proteins accumulate during treatment, and con centrations equivalent to about 3mg/l (about 1 to 2 per cent of the levels of unchanged di unisal) have been reported, although further accumulation is possible. The plasma protein adduct is eliminated in a biphasic fashion with a terminal half-life of about 10 days (McKinnon and Dickinson, 1989), possibly related to the turnover of protein. In the rat covalent binding slowly occurs in a variety of tissues (King and Dickinson, 1993), particularly in the bladder because of its exposure to high concentrations of the acyl glucuronide and a rearranged product of the glucuronide (Dickinson and King, 1993). The total resorption of di unisal acyl glucuronide from the bladder is, however, insigni cant, although the resorption of di unisal occurs readily (Dickinson and King, 1996). The covalent binding of drugs to proteins is considered as a potential cause of tissue toxicity and immunogenic reactions. The injection of adducts of di unisal with albumin leads to the production of circulating antibodies in the rat (Worrall and Dickinson, 1995) although only mild hypersensitivity reactions are associated with di unisal therapy (Cook et al. The clearance of di u nisal, like that of salicylate, is dose-dependent, and the accumulation is greater than predicted from a single dose. During multiple dosage the total plasma concentrations are about double that predicted, Figure 4. The acyl glucuronide is unstable, being hydrolysed back to di unisal, forming rearrangement products and covalent adducts with plasma proteins. The hydroxylated metabolite is largely excreted as an as yet unidenti ed conjugate. Rainsford but because of the saturable protein binding the unbound plasma concentrations increase to a greater extent. Thus, during dosage with 500mg di unisal twice daily, the unbound plasma concentrations are about 350 per cent of the plasma concentrations predicted from a single dose (Verbeeck et al. Because of the saturable metabolism and slow absorption the plasma concentrations are well sustained during long-term therapy, and the plasma concentrations during dosage with 1000mg once a day are little different from the concentrations at 500mg twice a day (Mojaverian et al. Sulphation is normally considered to be a high-affinity, low-capacity pathway, but in the case of di unisal the sulphation pathway is not saturable at therapeutic doses in man. The plasma clearance of di unisal decreases with decreasing renal function (Verbeeck et al. In rats preformed acyl glucuronide is rapidly hydrolysed, indicating that retention of the ester glucuronide and its subsequent hydrolysis back to di unisal is the cause of the apparently reduced clearance (Dickinson et al. By comparison, the phenolic glucuronide is stable and thus does not undergo this futile cycling (Brunelle and Verbeeck, 1997). There have been few studies on the effects of other factors or drugs on the pharmacokinetics of di unisal. Parallel with salicylate, there may be the in uence of sex hormones on the kinetics of di u nisal. The clearance of di unisal is about 60 per cent higher in men than in women, and is elevated to a similar extent in women by oral contraceptives (Macdonald et al. Smoking increases the clear ance of di unisal by about 35 per cent, possibly by induction of the minor hydroxylation pathway. In cirrhosis, the unbound clearance of di unisal is decreased by about one-third because of impairment of the glucuronidation pathways (Macdonald et al. Pro-drugs of diflunisal As is the case with salicylate, acyl esters of di unisal have been prepared with the aim of decreasing the gastrointestinal toxicity of di unisal and producing selective inhibitors of platelet aggregation. As with the salicylate esters, all the di unisal esters are hydrolysed readily with the lipophilic ester, the acetyl ester showing the greatest extraction by the rat liver (Hung et al. The stability of the con jugates of di unisal must be considered in the assay of these conjugates. The phenolic glucuronide is stable except at very low pH, but the acyl glucuronide is unstable at pH values above 4. Although salicylamide has little pharmacological activity, it has been used as model drug in pharmacokinetic and metabolic studies. The plasma concentrations of salicylamide are consider ably lower than those achieved by equivalent doses of sodium salicylate because of the rst-pass meta bolism of salicylamide and its more extensive tissue distribution resulting from lesser binding to plasma proteins (Seeberg et al. Absorption Although well absorbed from the gastrointestinal tract, salicylamide undergoes a variable degree of rst-pass metabolism. The extent of rst-pass metabolism is dose-dependent, with high rst-pass metabolism and very low plasma concentrations after small doses and substantive plasma concentra tions after doses of 1 to 2g (Barr et al. Under such circumstances the formulation becomes a critical variable, because a slow-release form should provide lower concentrations at rst-pass meta bolic sites than those produced by a rapid-release preparation. The result should therefore be a greater rst-pass metabolism after the slow-release form. Consistent with this prediction, the plasma concentra tions of salicylamide after an oral dose of 1. The extent of rst-pass metabolism also depends on the liver blood ow, the fractional absorption decreasing with increasing perfusion. Elimination the amide group of salicylamide is unaffected by metabolism and therefore salicylate is not a metabol ite, but the aromatic ring and phenolic group are modi ed in a similar fashion to salicylate (Figure 4. Salicylamide is mainly eliminated in man by transformation to the phenolic glucuronide and sul phate (Becher et al. The phenolic glucuronide is analogous to the phenolic glu curonide of salicylate, but the sulphate conjugate of salicylate has never been de nitely identi ed in Figure 4. A metabolite hydroxylated in the 3 position, 2,3-dihydroxybenzamide, has also been identi ed in the mouse. As is the case with salicylate, hydroxylation of salicylamide also occurs, but only small proportions of the drug are converted to gen tisamide (the analogue of gentisate) and from this to its glucuronide (Song et al. Hydroxylation to the 2,3-dihydroxybenzamide followed by glucuronidation has also been identi ed in mice (Howell et al. Like salicylate, the metabolism of salicylamide is saturable and the proportion of minor metabolites increases as the major pathways become saturated; thus the production of gentisamide is signi cant in man only when the formation of the sulphate is saturated (Levy and Matsuzawa, 1967). The availabil ity of inorganic sulphate controls the relative proportions of the metabolites. Both in man in vivo and in isolated rat hepatocytes, sulphoconjugation is enhanced while glucuronide formation is suppressed if the availability of sulphate is increased (Levy and Matsuzawa, 1967; Koike et al. From studies in rat hepatocytes, the relative production of the sulphate conjugate is favoured at low concentrations because of the relevant kinetic parameters of this pathway. Because of the lower Km value for the sulphoconjugation, this process is favoured over glucuronidation at low salicy lamide concentrations. An interesting aspect of the metabolism of salicylamide has been demonstrated in the perfused rat liver. The sequential metabolism of salicylamide is not identical to the metabolic pattern of a pre formed metabolite. As discussed above, salicylamide is hydroxylated to gentisamide and then glu curonidated. By comparison, preformed gentisamide is primarily sulphated at both the 2 and 5 positions to yield gentisamide, and is glucuronidated only when the higher-affinity sulphation pathway is saturated (Xu et al. Possibly, the glucuronidation of the metabolically formed gentisamide is favoured because of the occurrence of both oxidation and glucuronidation processes on the endoplas mic reticulum in the liver. Apart from its biotransformation in the liver, salicylamide is extensively metabolised in the intestine in the rabbit (Barr and Riegelman, 1970; Barr et al. Data obtained in the rat indicate that signi cant rst-pass metabolism of salicylamide occurs both in the small intestine and liver, with the greater extraction in the liver (Xu et al. Meta bolism also occurs in the kidneys, lung and forelimbs of dogs, particularly at low doses, and the lung may contribute to the high rst-pass metabolism of low doses of salicylamide (Fielding et al. Like salicylamide, ascorbic acid is metabolised in part to a sulphate conjugate, and ascorbic acid has therefore been used to explore the determinants of the formation of salicylamide sulphate. Orally administered ascorbic acid markedly decreases the formation of salicylamide sulphate in man and rats, whereas intravenous administration of the vitamin has little or no effect in rats (Houston and Levy, 1976). Similarly, the oral administration of sulphate, but not its intravenous infusion, decreases the oral availability of salicylamide in the dog, indicating a local effect of sulphate on the intestinal rst-pass metabolism of salicylamide (Waschek et al. Interactions between salicylamide and salicylates have been detected, although the mechanisms are unclear. The formation of both the sulphate and glucuronide conjugates of salicylamide is inhibited by salicylate and paracetamol (Levy and Yamada, 1971).
The risk of hypokalaemia erectile dysfunction drugs reviews order discount zenegra online, which may occur with both thiazide and loop diuretics erectile dysfunction va benefits generic 100 mg zenegra fast delivery, depends more on the duration of action than on potency and is thus greater with thiazides than with loop diuretics (when given in equipotent doses) treatment of erectile dysfunction in unani medicine order 100mg zenegra overnight delivery. Other electrolyte disturbances include hypercalcaemia (thiazides) erectile dysfunction treatment austin tx cheap zenegra amex, hypocalcaemia (loop diuretics) and hypomagnesaemia (thiazide and loop diuretics) erectile dysfunction medication names order zenegra 100 mg otc. Cardiovascular Drugs 71 Symptoms of fluid and electrolyte imbalance include dry mouth erectile dysfunction risk factors generic 100 mg zenegra amex, thirst, gastrointestinal disturbances (including nausea, vomiting), weakness, lethargy, drowsiness, restlessness seizures, confusion, headache, muscle pains or cramps, hypotension (including postural hypotension), oliguria, arrhythmias. The elderly are more susceptible to electrolyte imbalance than younger patients; treatment should begin with a lower initial dose of the diuretic (commonly about 50 % of the adult dose) and then adjusted carefully according to renal function, plasma electrolytes and diuretic response. Acetazolamide Tablet, 250 mg Capsule (s/r), 500mg Powder for injection, (sodium), 250mg, 500mg in vial Indications: reduction of intra-ocular pressure in open-angle glaucoma, secondary glaucoma, and peri-operatively in angle-closure glaucoma (see section 15. Cautions: elderly; pregnancy; breastfeeding; diabetes; pulmonary obstruction; monitor blood count and electrolytes if used for long periods. Contraindications: hypersensitivity to sulfonamides; chronic angle-closure glaucoma, hypokalaemia, hyponatraemia, hyperchloraemic acidosis; renal and hepatic impairment. Side effects: nausea, vomiting, diarrhea, taste disturbance; loss of appetite, paraesthesia, flushing, headache, dizziness, fatigue, irritability, depression; thirst, polyuria; reduced libido; metabolic acidosis and electrolyte disturbances on long-term therapy; occasionally drowsiness, confusion, hearing disturbances, urticaria, melaena, glycosuria, haematuria, abnormal liver function, renal calculi, blood disorders including agranulocytosis and thrombocytopenia, rashes including Stevens-Johnson syndrom and toxic epidermal necrolysis; transient myopia reported. Note: sustained release capsule is not recommended for treatment of epilepsy Storage: store at room temperature. Contraindications: hyperkalaemia, renal failure, and hypersensitivity; see also Hydrochlorothiazide Side effects: except for hyperkalaemia serious adverse effects are uncommon; nausea, anorexia, abdominal pain and flatulence, headache, weakness and dizziness. Rarely visual disturbances, blood dyscrasias, skin rashes, pruritus, bladder spasm, muscle cramps and jaundice. Dose and Administration: Edema: Oral: Adult: 5-10mg/day (up to 20mg) Elderly: initial: 5mg once daily or every other day. Cardiovascular Drugs 73 Amiloride and Hydrochlorthiazide Oral solution, 5mg + 50mg/5ml Tablet, 2. Cautions: children, elderly patients, pregnancy (not used to treat hypertension in pregnancy) and breast feeding; hypotension; correct hypovolaemia before using in oliguria. It may cause hypokalaemia and hyponatraemia, aggravates diabetes mellitus and gout, liver failure, renal impairment, prostatic enlargement, porphyria. Contraindications: patients with precomatose states associated with liver cirrhosis, renal failure with anuria. Side effects: hyponatraemia, hypokalaemia, hypomagnesaemia, hypochloraemic alkalosis, increased calcium excretion, hypotension, less commonly nausea, gastro-intestinal disturbances, hyperuricemia and gout, hyperglycemia, temporary increase in plasma cholesterol and triglyceride concentrations, photosensitivity and bone marrow depression, pancreatitis, tinnitus and deafness, orthostatic hypotension as a result of massive diuresis (dizziness or light-headedness when getting up from sitting position). Dose and Administration: Edema: Oral: Adult: initially 40 mg daily on rising, maintenance, 20 mg daily or 40 mg on alternate days, may be increased to 80 mg daily in resistant oedema; Child: 1 3 mg/Kg body weight daily (maximum 40 mg daily). Storage: Store at room temperature in a well closed container, protect from freezing and light. Hydrochlorothiazide Tablet, 25 mg Indications: oedema, hypertension and cardiac failure. Cautions: paediatrics, elderly patients, during pregnancy and breast-feeding, heart failure, aggravates diabetes and gout, and may exacerbate systemic lupus erythematosus, dyslipidaemia. Side effects: postural hypotension and mild gastrointestinal effects, impotence (reversible), hypokalaemia, hypomagnesaemia, hyponatraemia, hypercalcemia, hypochloraemic alkalosis, hyperuricemia, gout, hyperglycemia, and increased in plasma cholesterol concentrations, less commonly rashes, photosensitivity, blood disorders (including neutropenia and thrombocytopenia), pancreatitis, intrahepatic cholestasis, hypersensitivity reaction. Edema: Oral: Adult: initially 25 mg daily on rising increasing to 50 mg daily if necessary, elderly initially 12. Severe Oedema in patients unable to tolerate loop diuretics: Oral: Adult: up to 100 mg either daily or on alternate days (maximum 100 mg daily). Mannitol Injection, 25 % in 50 ml, 20 % in 250 ml, 10 % in 500 ml Indications: oliguria due to acute renal failure; reduction of intracranial pressure cerebral oedema; reduction of intraocular pressure for angle closure glaucoma. Contraindications: cardiac failure, pulmonary oedema, well established anuria caused by severe renal disease or impaired renal function who do not respond to a test dose, severe dehydration, metabolic edema, intracranial bleeding. Side effects: chest pain or fast heartbeat, chills or fever, head ache, convulsions, difficulty in urination, electrolyte imbalance (confusion, irregular heartbeat, muscle cramps or pain, numbness, tingling, pain or weakness in hands or feet), pulmonary congestion, thrombophlebitis (redness or swelling or pain at injection site). Dose and Administrations: Test dose (to assess adequate renal function), by intravenous infusion, as a 20 % solution, 200 mg/kg body weight infused over 3-5 minutes, repeat test dose if urine output less than 30 50 ml/hour; if response inadequate after second test dose, re-evaluate patient. Side effects: as for hydrochlorothiazide, and also palpitation, chest pain, and chills. Cardiovascular Drugs Spironolactone Tablet, 25 mg, 100 mg Indications: oedema and ascites in cirrhosis of the liver, malignant ascites, nephritic syndrome, congestive heart failure; primary hyperaldosteronism. Side effects: gastro-intestinal disturbances; impotence, gynaecomastia, menstrual irregularities; lethargy, headache, confusion; rashes, hyperkalaemia (discontinue), hyponatraemia, hepatotoxicity, osteomalacia, and blood disorders reported. Dose and Administration: Oral: Oedema: Adult: 100 200 mg daily, increased if necessary to 400 mg daily in resistant oedema, usual maintenance dose 75 200 mg daily, Child: initially 3 mg/kg body weight daily in divided doses. Primarily hyperaldosteronism: Adult: diagnosis, 400 mg daily for 3 4 weeks; preoperative management, 100 400 mg daily; if not suitable for surgery, lowest effective dose for long term maintenance. Storage: at room temperature in a tight, light resistant container 2. Sclerosing Agents Sclerosants are used in the managment of varicosities including varicose veins and oesophageal varices when their capacity to damage veins is apparently put to good use. The mechanisms by which injection sclerotherapy works are not completely understood but are thought to involve damage to the intima, intraluminal thrombosis, and intravascular fibrous organisation. Sclerosants used include: ethanolamine oleate, sodium tetradecyl sulphate and sodium morrhuate. Ethanolamine Oleate Injection, 5 % in 2 ml ampoule Indications: treatment of varicose veins and oesophageal varices. Cautions: fatal anaphylactic shock has been reported following administration; use with caution and decrease dose in patients with significant liver dysfunction, with concomitant cardiorespiratory disease, or in the elderly or critically ill. Contraindications: varicose veins of the legs in patients with thrombosis or a tendency to thrombosis; acute phlebitis, marked arterial, cardiac, or renal 2. Cardiovascular Drugs 77 disease; local or systemic infections; or uncontrolled metabolic disorders such as diabetes mellitus. Side effects: irritant to skin and mucus membranes; local injection may cause sloughing, ulceration, and in severe cases, necrosis and pain may occur at the site of injection. Patients receiving treatment for oesophageal varices may develop pleural effusion or infiltration. Morrhuate Sodium Injection, 5% in 5ml ampoule Indications: treatment of small, uncomplicated varicose veins of the lower extremities. Contraindications: hypersensitivity reactions to the drug or to the fatty acids of cod liver oil. Side effects: thrombosis, valvular incompetency, vascular collapse, drowsiness, headache, dizziness, urticaria, nausea, vomiting, burning at the site of injection, severe extravasation effects, asthma, anaphylaxis, weakness. Sodium Tetradecyl Sulphate Injection, 1 % in 2 ml ampoule, 3 % in 2 ml ampoule and 5 ml vial. Drugs used in vascular shock Shock is a complex clinical syndrome of multiple aetiologies but the common factor in all types of shock is a failure of the circulatory system to maintain celluar perfusion and function. Cardiac shock usually results from acute failure of the heart, leading to an inadequate stroke volume and reduced cardiac output. It has a number of causes, but is most commonly associated with acute myocardial infarction. Successful correction of hypovolaemia may alleviate hypotension in some cases, but cardiac out put may remain depressed and signs of impaired organ perfusion may persist, necessitating additional therapy. In cardiogenic shock cardiac output is usually low but peripheral resistance is high and drugs that have predominantly inotropic effects are most suitable. Dopamine has been widely used in all forms of shock, often in combination with other inotropes. At low doses it causes peripheral vasodilation, which was thought to protect renal perfusion; however, any clinical benefit is unclear and at higher doses it causes vasoconstriction and is useful where hypotension is not significant. Noradrenaline causes peripheral vasoconstriction and should be reserved for severe hypotension. It is particularly useful in septic shock where the cardiac output is usually high but peripheral resistance is low. Adrenaline has also been used alone but renal artery vasoconstriction may limit its use, and it has also been reported to cause lactic acidosis. In cardiogenic shock associated with myocardial infarction, specific therapy to restore myocardial perfusion is also indicated. Drug interactions: other sympathomimmetic agents (additive effects), alpha adrenergic blocking agents, anaesthetics (volatile), beta blockers, digoxin, theophylline, tricycluc antidepressants, monoamine oxidaze inhibitors. Side effects: tachycardia and arrhythmia, hypertension, hypotension, tremor, anxiety, sweating, nausea, vomiting, weakness, dizziness, pulmonary oedema, headache, peripheral vasoconstriction. Dose and Administration: the 1:1000 (1mg/ml) concentration of epinephrine injection must be diluted before administering intravenously. The dose may be titrated up to 2 to 10microgram per minutes for desired hemodynamic response. Dobutamine Powder for injection, 250 mg in vial Indications: inotropic support in cardiogenic shock, acute myocardial infarction, post-cardiac surgery and septic shock after adequate volume replacement; management of refractory cardiac failure. Cautions: pregnancy, severe hypotension, hypovolaemia should be corrected before treatment. Contraindications: idiopathic hypertrophic cardiomyopathy with outflow obstruction. Side effects: palpitations, ectopic heartbeats and, rarely, ventricular tachycardia, angina, increase in systolic blood pressure (10 20 mmHg, in most patient, but may be more dramatic, particularly in the presence of preexising hypertension), nausea, vomiting, headache, paraesthesia and dyspnoea may occur. May be infused for up to 72 hours, provide the patient is carefully monitored; thereafter intermittently. Dopamine Hydrochloride Injection, 40 mg/ml in 5 ml ampoule Indications: cardiogenic shock in infarction or cardiac surgery, renal failure or septicaemia after adequate volume replacement; short-term management of refractory cardiac failure and treatment of acute hypotension. Cautions: hypovolaemia; low dose in shock due to acute myocardial infarction, hypoxia, hypercapnia, and metabolic acidosis before or at some time as starting treatment, history of peripheral vascular disease, elderly. Note: hypovolaemia should be corrected before dopamine is used in shocked patients. Drug interactions: halogenated anaesthetics (such as cyclopropane, halothane); monoamine oxidase inhibitors, betablockers, digoxin, ergotamine/ergotamine, tricyclic antidepressants. Contraindications: tachyarrhythmias, ventricular fibrillation, ischaemic heart disease, Pheochromocytoma; hyperthyroidism. Side effects: nausea and vomiting, peripheral vasoconstriction, hypotension with dizziness, fainting, flushing, tachycardia, ectopic beats, palpitations, anginal pain; headache dyspnoea, hypertension. V infusion into large vein: Adult: initially 2 5 micrograms/Kg/minutes; gradually increased by 5 10 micrograms/Kg/minutes according to blood pressure, cardiac output and urine output; seriously ill patients up to 20 50 micrograms/Kg minutes. Cautions, Drug interactions, Contraindications and Side effects; as for adrenaline above. Levarterenol (Noradrenaline) Tartarate Injection 8mg/ml in 1ml ampoule Indications: treatment of shock which persists after adequate fluid volume replacement. Cautions: never use leg veins for infusion sites, monitor blood pressure closely and adjust infusion rate, hypoxia or hypercapnia. Contraindications: hypersensitivity to the drug, pregnancy, during anesthesia with cyclopropane or halothane anesthesia (risk of ventricular arrhythmias) Side effects: bradycardia, arrhythmia, peripheral ischemia, headache, anxiety, and dyspnea, skin necrosis, respiratory difficulty. Cardiovascular Drugs 81 Note: Noradrenaline is administered only by intravenous infusion. Subcutaneous or intramuscular administration is not recommended because of the potent vasoconstrictor effect of norepinephrine. Phenylephrine Hydrochloride Injection, 10 mg/ml in 1 ml ampoule Indications: treatment of vascular failure, unresponsive to adequate fluid volume replacement, in shock, shock like states, drug induced hypotension, or hypersensitivity. Cautions: late pregnancy and during labour, diabetes mellitus, cerebral arterioscerosis, bradycardia, elderly patients. Side effects: chest discomfort, pain, dizziness, nervousness, restlessness, trembling, troubled breathing, unusual paleness, and unusual weakness. Thrombolytic agent Antithrombic enzymes convert plasminogen to plasmin, which inturn degrades fibrin thrombi and fibrinogen. The most generally accepted indication for the use of antithrombic enzymes is in the treatment of selected cases of acute myocardial infarction. Other indications include acute severe pulmonary thromboembolism; acute arterial thrombosis and thromboembolism; severe deep-vein thrombosis; and clearance of ateriovenous catheters and cannulae. Drug interactions: aminocaproic acid, oral anticoagulants, heparin, non steroidal ant inflammatory drugs, nitroglycerin. Contraindications: cerebrovascular accident, or history of recent major trauma, surgery or head injury (within the preceding month); gastrointestinal bleeding within the last month; dissecting aneurysm, intracranial aneurysm, active bleeding or known bleeding disorder. Storage: store at room temperature or under refrigeration; once reconstituted it must be used within 8 hours. If reconstituted and not used immediately, store in refrigerator and use within 8 hours. Antitussives/Expectorants Cough is an important physiological protective mechanism, but may also occur as a symptom of an underlying disorder such as asthma, gastro-oesophageal reflux disease, and postnasal drip. Treatment of the disorder often alleviates the cough, but there are times when symptomatic treatment is appropriate. The treatment chosen depends on whether the cough is productive or non productive. A non-productive cough such as that often seen with the common cold serves no useful purpose for the patient, and cough suppressants may provide some relief, particularly if given at night. Of the commonly used cough suppressants, pholcodine and dextromethorphan are considered to have fewer adverse effects than codeine. Codeine or similar opioids are not generally recommended as cough suppressants in children, and should be avoided altogether in those under 1 year of age. A productive cough is characterized by the presence of sputum and may be associated with conditions such as chronic bronchitis, bronchiectasis, or cystic fibrosis. Cough suppressants are inappropriate, since the cough serves the purpose of clearing the airways; expectorants such as guaifenesin have been used on the grounds that increasing the volume of secretions in the respiratory tract facilitates removal by ciliary action and coughing. Mucolytics such as carbocisteine have been shown to affect sputum viscosity and structure and patients with productive cough have reported alleviation of their symptoms, but no consistent improvement has been demonstrated in lung function. Carbocisteine Syrup, 2%, 5% Indications: for its mucolytic activity in respiratory disorders associated with productive cough.

Please meet at 8:15 am in the Family Hospitality Suite erectile dysfunction kamagra effective zenegra 100 mg, located in the Republic Room on the 4th foor of the Auxiliary Registration / Grand Hyatt San Antonio erectile dysfunction protocol free ebook generic 100 mg zenegra visa. Upon arriving at the museum erectile dysfunction rings order zenegra now, a knowledgeable docent will guide the group through the museum giving an overview of the exhibits erectile dysfunction vascular causes zenegra 100 mg otc. There are Conference Registration also thousands of permanent pieces of art covering over 5 erectile dysfunction pump walgreens best 100 mg zenegra,000 years of history around the Henry B impotence by smoking order zenegra american express. Please meet at 9:45 am in the Family Hospitality Suite, located in the Republic Room on the 4th foor of the Grand Hyatt Auxiliary Registration / Family Hospitality Suite* San Antonio. Los Barrios has received numerous awards and Conference Registration has become a San Antonio tradition. Gonzalez Convention Center create before you, but also take the recipes home with you. We will be taking a bus to the restaurant, so please meet at 11:30 am in the Auxiliary Registration / Family Hospitality Suite, located in the Republic Room on the 4th foor of the Grand Hyatt Family Hospitality Suite* San Antonio. Discussions career, representing private practice, academics, hybrid practice and 4th will focus on details of private practice versus academics, contract analysis, year fellowships, who will briefy share their story and then take questions networking skills, negotiating skills, and work-life balance. This luncheon is available to all trainees in gastroenterology and hepatology, Advance registration is required and space is limited. Visit the Registration Desk in the Level) for registration information, however, this event may be sold out. The top scoring fellows from each year were then regarding the future of their medical careers. Join us in the Hands-On female subspecialist, balancing career and family, and opportunities for Workshop area of the Exhibit Hall to cheer on the competitors. Visit the Registration Desk in the Main Monday, October 28, 2019 Lobby (Street Level) for registration information, however, this event may be sold out. Watch expert faculty demonstrate the Exhibit Hall, and will be open when the Exhibit Hall is various endoscopic procedures, and try out the latest products open. Edward Berk Distinguished Lecture is awarded to individuals prominent in gastroenterology or a related area. The lectureship was such as the medical home, for the management of infammatory bowel disease when established in recognition of the signifcant contributions made by J. Recently, he University of Arizona and a Fellowship in Gastroenterology at the Mayo Clinic, has been involved in developing new models of healthcare, including the frst-of-its before joining the faculty at Mayo Rochester in 1999. Sun in Rochester, where he has previously served as Director of the Pancreas Clinic. He is past Councilor and President of the American Pancreatic Association Each year, a lecturer with a distinguished background in gastroenterology or an allied feld is and International Association of Pancreatology. He co-leads the Diabetes-Pancreatic Cancer Working Learn how to appreciate the diverse clinical presentations of celiac disease, recognize Group in the U01. Kelly presents, Celiac Disease: Society, and the Old Dominion Society of Gastroenterology Nurses and Associates, is in honor of Myths and Mysteries. Graham Lecture, and gain a better on disease pathogenesis, diagnosis, and new treatment approaches. His postdoctoral training more than 250 clinical and basic original research articles, as well as book chapters and included an internship and residency in internal medicine, as well as a fellowship in invited reviews appearing in medical and scientifc journals, including the American gastroenterology, at the University of Chicago. Kirsner Chair Journal of Gastroenterology, the Journal of Clinical Investigation, Gastroenterology, the Professor of Medicine and was Chief of the Section of Gastroenterology, Hepatology Lancet and the New England Journal of Medicine. He is a member of several professional societies Post-Colonoscopy Colorectal Cancer: How Are We Doing He has served as a Member and Chair of the the risk of post-colonoscopy colorectal cancer in clinical practice when Dr. Linda Rabeneck, a gastroenterologist, clinician scientist, and health care Bowel Disease. He is former Editor-in She is a Professor of Medicine at the University of Toronto and Senior Scientist at the Chief of Nature Clinical Practice Gastroenterology & Hepatology and served as Associate Institute for Clinical Evaluative Sciences also in Toronto. Cohort Phenomenon of Peptic Ulcer Gallstone Formation: Romancing the Stone 2008 Christopher C. The Latest Data and Insights Drug-induced Liver Injury: What Have We Adenocarcinoma Moved from the 2017 Corey A. Young Adults With Adenomas: How Does Their Risk for Metachronous Advanced Adenomas Compare With Older Adults Posters receiving both a named Category Colorectal Cancer Prevention or category award plus a Presidential Poster Award are Joseph C. Optimizing Inpatient Management of Acute Pancreatitis: Lymph Nodes A Single Center Quality Improvement Project Category Interventional Endoscopy 1 1 Category Biliary/Pancreas Irina M. Efficacy of Biofeedback Therapy for Dyssynergic Constipation Characterization: Is There Any There There Among Elderly Patients Category Small Intestine 1 2 Category Functional Bowel Disease Ryan C. Human Milk Oligosaccharides Improve All the Central Symptoms of Celiac Disease of Irritable Bowel Syndrome: A Multi-Center, Open Label Trial Category Small Intestine Olafur S. Intrinsic Sex-Specific Differences in Inflammatory and Fibrotic Gene Expression and Remodeling Contribute to Male Disease Predisposition in Eosinophilic Esophagitis Quan M. The Effect of Deep Sedation on Adenoma Detection Rate in this award is determined by the Abstract Selection Committee. University1 1 1 Reliably Detects Polyps Earlier Than Physicians During Colonoscopy Susan Y. Vedolizumab-Induced Remission of Refractory Microscopic Colitis: A Single Institution Case Series P0330. Takeda Gastrointestinal Bleeding While on Warfarin vs Direct Oral Anticoagulants 1 1 2 Development Center Americas, Inc. Epidemiology of Major Depressive Disorder, Anxiety Disorder, and Bipolar Disorder in Ulcerative Colitis in the United States Between 2014 P0574. Academic Medical Center, Varices in Cirrhotic Patients Amsterdam, Noord-Holland, Netherlands; 2. Epidemiology of Diverticulitis and Prevalence of First-Ever and Technical Reviews Colorectal Cancer Post-Diverticulitis in Adults in the United States Daniel W. Eosinophilic Esophagitis Presenting With Esophageal Wall Dissection of Clostridioides difficile Infection Joshua D. Cleveland Clinic, Abu Dhabi, Abu Dhabi, With Treatment Satisfaction but Is Inadequately Practiced United Arab Emirates Joy W. Center for Esophageal Diseases and Swallowing, University of North Carolina, P1293. Percutaneous Transhepatic Single-Operator Cholangioscopy With Variceal Band Ligation Electrohydraulic Lithotripsy in the Management of Intrahepatic Stones in a Jason R. Hormones: A Systematic Review and Meta-Analysis Singapore General Hospital, Singapore, Singapore; 8. Increased Risk of Sessile Serrated Adenomas on Initial Screening Ampulla of Vater in the Pylorus Colonoscopy in Post-Bariatric Surgery Patients Nathan L. Adjunctive Yield of Wide-Area Trans-Epithelial Sampling With Haplotypes Across Ethnicities and Regions in the United States Computer-Assisted Three-Dimensional Analysis in Detection of Dysplasia Molly R. Raphael, Molly Stewart1 2, Divyesh Sejpal, Mary Cheung1 2, Matthew Mountain, PhD3, Peter H. Tradipitant Complete Responder Analysis in Gastroparesis Patients Ovarian Abscess via a Lumen-Apposing Metal Stent Jesse L. This important and the multi-faceted pressures of new and increasing scientifc evolving educational need must be met in a way that touches on the developments, pressures from payors and policymakers, and demands impact of various forms of cancer on the overall health and quality of by more knowledgeable patients mandate that gastroenterologists fnd life of these patients. Obesity has drastically increased in prevalence in the United States, Declining reimbursement, increased demand for measurement of from less than 15% in the 1960s to over 30% at present. It has been quality, and an insufcient workforce also remain signifcant challenges predicted that if the rates continue at their current pace, by 2015, 75% for gastroenterologists and their practices. Therefore, not only is it imperative important to identify more efcient ways to obtain the latest scientifc for gastroenterologists to be knowledgeable regarding obesity knowledge and institute scientifcally sound therapy so that the highest prevention and treatment options, but it is also important that they quality of patient care can be maintained. Specifcally, endoscopic techniques and advancements in diagnosis and treatment options, as well as on the management options in these patients can be a challenge. Education regarding optimizing the cancerous polyps or diagnose cancers at an early stage. Increasing the rate of patient participation in colorectal cancer screening and surveillance is also important. Often, the gastroenterologist of fat lesions, is a need that afects gastroenterologists. In addition, relies on the expertise of the hepatologist to assist in the management it is important that gastroenterologists understand the importance of of these patients; however, with hepatologists operating at capacity, grading bowel preparation using a validated scale, and that they are the gastroenterologist must be able to ofer the best quality of familiar with recommendations for the timing of a repeat colonoscopy care and treatment options to patients with liver disease. The serrated pathway, Hepatitis C will be the most dramatically changing area of liver disease which may account for at least 15% of all colorectal cancers, requires over the next few years, and there will be two major areas that will gastroenterologists to understand the challenges in detection, resection, require focus and attention. Also, within the next 1-2 years, therapy will incidence and has been the subject of intense research leading to recent likely be completely all-oral, interferon-free, and perhaps even ribavirin clinical guidelines. There will be a series of new regimens available, with new ones and this feld has dramatically changed in the past several years due being introduced at a very rapid pace. With Pancreaticobiliary diseases can also be extremely challenging to manage, guidelines published on gastroesophageal refux disease, eosinophilic and can vary greatly in complexity and severity. Gastroenterologists esophagitis, and achalasia within the last year, this has been an play an essential role in both the evaluation and the management of active area and this new information needs to be disseminated to the patients with pancreaticobiliary disorders. As endoscopic diagnostic and therapeutic areas in gastroenterology creates a need technology advances, patients are simultaneously becoming more to communicate the latest techniques and strategies for managing complex, making it essential that gastroenterologists are up-to-date everything from patients with altered anatomy to identifcation and on these management techniques and strategies. Education on the removal of large and difcult polyps to developing practice of natural diagnosis and management of various forms of pancreaticobiliary disease orifce transluminal endoscopic surgery. Gastroenterologists in a variety including pancreatitis, pancreatic cysts, pancreatic cancer, and biliary of practice settings need to learn and integrate these new therapies into disorders is critical to obtaining the best patient outcomes. Practice efciency is also of great group of patients who have been among the most difcult to treat. Ever-expanding access to information on a real-time basis condition, infammatory, or infectious process, gastroenterologists must be by both clinicians and patients provides unique opportunities as well as aware of the various potential causes of diarrhea and the most appropriate challenges to the healthcare delivery system. Safeguards against commercial bias have been put afects 20% of American adults on a weekly basis. Anyone who refuses to disclose relevant fnancial its pathophysiology, diagnosis, treatment options, and complications relationships will be disqualifed. While less relevant fnancial relationships to the learners prior to the beginning of common, eosinophilic esophagitis appears to be increasing markedly in an education activity. Vice Chair, Board of Governors the Accreditation Council for Continuing Medical Education Patrick E. Experts will review the underlying 7:00 am Welcome and Introductions causes and clinical implications of commonly encountered diseases Darwin L. Lecture presentations will be followed by interactive Testing in the Management of Esophageal Disorders question and answer sessions. The course faculty are recognized experts impedance planimetry, and pH testing in the assessment of in their felds and pioneers in better understanding of the disease patients with esophageal disorders. Explain the mechanisms behind novel diagnostic strategies and pharmacologic approaches for patients with celiac disease. Physicians 10:15 am How to Apply Molecular and Genetic Testing to Colon should claim only the credit commensurate with the extent of their Polyps and Cancer Management participation in the activity. Anyone who refuses to disclose relevant Consultant: Ariel Precision Medicine fnancial relationships will be disqualifed. Salix/Valeant Pharmaceuticals Consultant: Allergan Pharmaceuticals, Ironwood, Salix/Valeant Renee L. Speakers Bureau: Allergan Pharmaceuticals, Ironwood, Salix/Valeant Pharmaceuticals Peter H. Physicians 3:10 pm Q & A should claim only the credit commensurate with the extent of their 3:25 pm Break participation in the activity. Thomas has indicated no relevant 3:00 pm Panel Presentations: 10 Things You Need to Know from Clinical Assistant Professor, University of a Business Standpoint fnancial relationships. Partner, Rockford Gastroenterology practice (both traditional and clinical track), employed Associates Ltd. Wilson has indicated no relevant fnancial 4:40 pm Course Wrap-Up and Closing Remarks relationships. Leavitt has indicated no relevant fnancial To resolve identifed conficts of an education activity (including their spouse or partner) are required relationships. Clarke has indicated no relevant United Digestive; Executive Committee fnancial relationships. Flamm has indicated no relevant Partner Physician, Austin Partner; Digestive Health Associates relationships.
Buy zenegra 100 mg visa. Erectile Dysfunction Treatments ★★ Top 10 Natural ED Treatments ★★.